

서론
만성콩팥병(chronic kidney disease)의 유병률은 나라마다 다양하게 보고되고 있다. 미국의 경우 만성콩팥병 3∼4단계의 유병률이 1990년대부터 2000년대까지 증가하는 추세였으나 2000년대 이후로는 큰 변화를 보이지 않고 있고[1,2], 영국에서는 2000년대 들어서 만성콩팥병 3∼5단계의 유병률이 오히려 감소하였다[3]. 우리나라의 경우 코로나바이러스병-19 (coronavirus disease 2019) 유행이 시작하였던 2020년을 제외하고는 2007년부터 2019년까지 추정사구체여과율 60 mL/min/1.73 m2 혹은 단회 소변검사에서 단백뇨 양성으로 정의된 만성콩팥병의 유병률은 점진적으로 증가하는 경향을 보였지만(2007∼2010년 5.1%; 2017∼2019년 7.1%) [4], 2000년대 초반과 비교하면 만성콩팥병의 유병률은 오히려 감소하는 경향을 보였다[5,6]. 노르웨이에서도 2006∼2008년 만성콩팥병 1∼5단계의 유병률이 1995∼1997년 유병률과 차이가 없는 수치를 보였다[1,6].
이렇게 2000년대 이후로 선진국들에서 만성콩팥병의 유병률이 다소 둔화되는 경향이 보이고 있지만 그 정확한 이유는 불확실하다[1]. 아마도 이전보다 고혈압환자에서의 혈압조절이나 당뇨병환자에서의 혈당조절이 개선되어 왔기 때문이 아닌가 추정되고 있다[1,7]. 뿐만 아니라 안지오텐신전환효소억제제(angiotensin converting enzyme inhibitor)나 안지오텐신수용체차단제(angiotensin receptor blocker)와 같은 레닌-안지오텐신계억제제(renin-angiotensin system inhibitor)가 지난 수십여 년 동안 만성콩팥병 환자들에게 처방되면서 콩팥보호에 기여해 온 점도 언급하지 않을 수 없다[1,7,8]. 그러나 오랜 기간 만성콩팥병의 표준치료로 사용된 레닌-안지오텐신계억제제이지만 여전히 많은 만성콩팥병 환자들은 말기콩팥병(end-stage kidney disease)으로 진행하고 또 일부는 경과 중 심혈관질환으로 조기 사망하는 등 레닌-안지오텐신계억제제의 한계는 명확하였다[8,9]. 게다가 만성콩팥병의 유병률 자체는 발생률의 변화에 따라 둔화되는 경향을 보이고 있지만 인구 증가, 노령화 및 당뇨병 등 대사질환 유병자 증가 등으로 인하여 만성콩팥병 환자 수 자체는 오히려 늘고 있어서, 현재 전 세계 인구의 약 10%가 만성콩팥병을 앓고 있으며 가장 흔한 사망 원인 중 하나로 지적되고 있다[1]. 특히 우리나라는 당뇨병 유병자 그리고 노령인구 증가에 따라 신대체요법이 필요한 말기콩팥병 환자 수가 급격하게 증가 추세를 보이고 있다[10,11]. 그럼에도 불구하고 레닌-안지오텐신계억제제 외에는 만성콩팥병 치료제가 없었던 상황에서 정말 예상하지 못한 곳에서 새로운 만성콩팥병 치료제를 찾게 되었는데, 그것이 바로 SGLT2억제제(sodium glucose cotransporter 2 inhibitor)이다[12].
본론
1. 당뇨병콩팥병
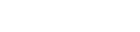
SGLT2억제제가 유럽과 미국에서 각각 2012년과 2013년에 사용 승인을 받았을 때 대부분의 신장전문의들은 단순한 혈당강하제 중 하나로 생각했었다[12]. 오히려 일부에서는 콩팥세관에 손상을 가할 수 있을까 우려했으며 특히 급성콩팥손상을 잠재적으로 유발할 가능성이 높다고 생각했다[12,13]. 그러나 그러한 걱정은 오래 가지 않았으며 오히려 임상시험을 진행하는 과정에서 SGLT2억제제에 예상하지 못한 콩팥보호의 효과가 있다는 사실을 알게 되었다[12,14]. 2015년 Empagliflozin Cardiovascular Out-come Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) 임상연구부터 2023년 The Study of Heart and Kidney Protection With Empagliflozin (EMPA-KIDNEY) 임상연구까지 지난 수 년여 동안 수행된 SGLT2억제제를 대상으로 한 주요 13개 임상시험들을 메타분석한 결과[15-17], 2형당뇨병이 동반된 대상자들 중 SGLT2억제제 치료에 배정된 경우 콩팥병 진행 위험이 38% 감소하였다(상대위험도 0.62, 95% 신뢰구간 0.56 to 0.68) [15]. 심지어는 SGLT2억제제를 사용하게 되면 당뇨병이 동반된 환자에서 급성콩팥손상의 위험을 21% 낮추었다(상대위험도 0.79, 95% 신뢰구간 0.72 to 0.88) [15]. Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE), Effect of Sotagliflozin on Cardiovascular and Renal Events in Patients with Type 2 Diabetes and Moderate Renal Impairment Who Are at Cardiovascular Risk (SCORED), Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) 그리고 EMPA-KIDNEY 임상연구 등 만성콩팥병 환자들을 주 대상으로 한 임상시험 4개를 메타분석한 결과[17-20], 콩팥병 원인이 당뇨병콩팥병으로 확인된 대상자들에서 SGLT2억제제를 투여하면 콩팥병 진행 위험이 40% 감소되었다(상대위험도 0.60, 95% 신뢰구간 0.53 to 0.69) [15]. 이러한 SGLT2억제제의 콩팥 이득을 예측 모델에 적용해보면 당뇨병이 동반된 1,000명의 만성콩팥병 환자에서 1년 동안 SGLT2억제제를 사용하면 11명에서 콩팥병 진행이 적게 생기고 급성콩팥손상이 4명에서 적게 생기며, 반면 케토산증과 하지 절단은 각 약 1명씩 발생하게 된다[15]. SGLT2억제제의 콩팥병 진행에 대한 보호효과는 알부민뇨가 많은 환자들에서 보다 크게 나타나지만 알부민뇨가 적거나 추정사구체여과율이 양호하더라도 당뇨병에서 SGLT2억제제 사용에 따른 콩팥 이득이 있음이 보고되고 있다[21,22]. 이러한 근거들을 바탕으로, Kidney Disease: Improving Global Outcomes (KDIGO)의 KDIGO 2022 만성콩팥병의 당뇨병관리 임상진료지침에서는 SGLT2억제제를 단순한 혈당강하제를 넘어 2형당뇨병 콩팥병의 일차선택약물로 격상시켰다[23]. 마찬가지로 대한신장학회 당뇨병콩팥병 진료지침에서도 2형당뇨병 콩팥병 환자에서 알부민뇨와 무관하게 추정사구체여과율 20 mL/min/1.73 m2 이상이라면 일차적으로 시작하고 신대체요법을 시작하기 전까지 지속하도록 권장하고 있다[23,24]. 한편, 알부민뇨는 있지만 정상 혈압인 당뇨병콩팥병 환자에서 레닌-안지오텐신계억제제 사용의 근거는 다소 부족하여 임상진료지침마다 권고 수준이 다르지만[23-25], 대한신장학회 당뇨병콩팥병 진료지침, KDIGO 2021 만성콩팥병의 혈압관리에 대한 임상진료지침과 KDIGO 2022 만성콩팥병에서의 당뇨병관리 임상진료지침 등에서 공통적으로 제시하고 있는 것은 당뇨병환자에서 만성콩팥병 1∼4단계이면서 알부민뇨가 동반된 경우 환자가 감내할 수 있는 혈압 범위 내에서 레닌-안지오텐신계억제제를 최대용량으로 사용하도록 권장하고 있다는 점이다. 당뇨병콩팥병 치료제로서의 레닌-안지오텐신계억제제의 적응증에는 알부민뇨가 포함되어야 한다는 점을 고려한다면, 알부민뇨가 정상 범위 내(소변 알부민-크레아티닌비 < 30 mg/g)인 2형당뇨병 콩팥병 환자에서는 SGLT2억제제가 유일하게 근거를 가지고 사용될 수 있는 콩팥병 치료제이다(Fig. 1).
Fig. 1.
Indications for initiating RAS and SGLT2 inhibitors in diabetic kidney disease. (A) Range of indications for initiating RAS inhibitors (red-colored boxes), and (B) SGLT2 inhibitors (blue-colored boxes) in diabetic kidney disease based on the KDIGO GFR and albuminuria categories for staging chronic kidney disease according to the KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease [23] and the KSN 2023 Practical Recommendations for the Management of Diabetic Kidney Disease [24] are shown. (C) SGLT2 inhibitors may be initiated in patients with diabetic kidney disease with a normal range of albuminuria if they have an eGFR ≥ 20 mL/min/1.73 m². The dosage of RAS inhibitors should be reduced or discontinued only as a last resort in chronic kidney disease patients with symptomatic hypotension, uncontrolled hyperkalemia, or uremic symptoms. Similarly, once an SGLT2 inhibitor is initiated, it should be continued even if the eGFR falls below 20 mL/min/1.73 m², unless it is not tolerated or kidney replacement therapy is initiated [22].
RAS, renin-angiotensin system; SGLT2, sodium glucose cotransporter 2; KDIGO, Kidney Disease: Improving Global Outcomes; GFR, glomerular filtration rate; KSN, Korean Society of Nephrology; eGFR, estimated glomerular filtration rate.

2. 비당뇨병 만성콩팥병
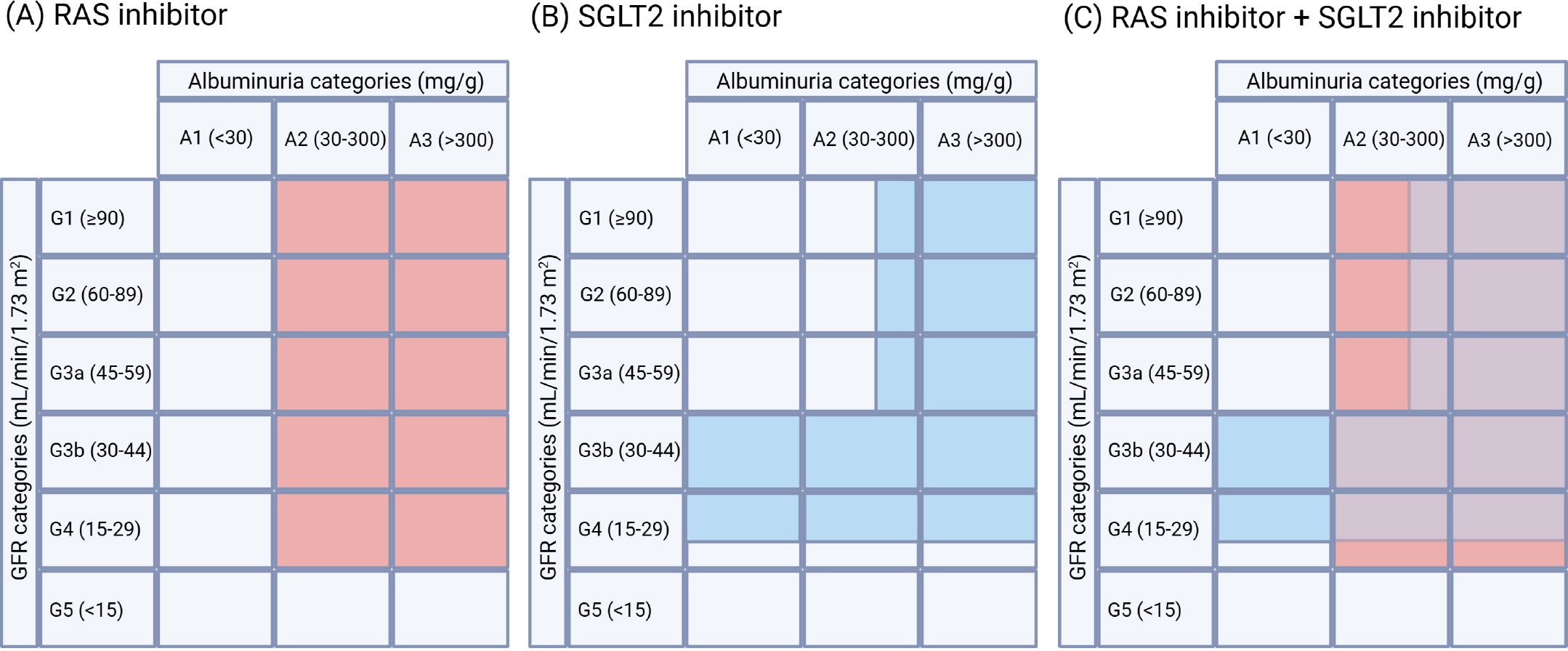
SGLT2억제제가 단순한 혈당강하제가 아니라는 근거는 비당뇨병 만성콩팥병 환자에서의 효과가 입증되었기 때문이다[15,22]. 당뇨병이 동반되지 않은 대상자들을 포함시킨 6개의 SGLT2억제제 임상시험들을 메타분석한 결과, 당뇨병이 없는 대상자들에서 SGLT2억제제의 투여는 콩팥병 진행 위험을 31% 감소시켰고(상대위험도 0.69, 95% 신뢰구간 0.57 to 0.82), 급성콩팥손상의 위험 역시 34% 낮추었다(상대위험도 0.66, 95% 신뢰구간 0.54 to 0.81) [15]. 특히 비당뇨병 만성콩팥병의 원인질환에 따라 분석해보면, SGLT2억제제는 허혈 및 고혈압콩팥병 환자군과 사구체질환 환자군에서 콩팥병 진행 위험을 각각 30% 및 40% 감소시켰다(각각 상대위험도 0.70, 95% 신뢰구간 0.50 to 1.00; 상대위험도 0.60, 95% 신뢰구간 0.46 to 0.78) [15]. 결과적으로 사구체질환 환자에서의 SGLT2억제제의 콩팥보호효과가 전체 비당뇨병 만성콩팥병에서 SGLT2억제제의 유의한 결과를 주도하였다. 그 중에서도 IgA신장병증(IgA nephropathy)에서의 SGLT2억제제의 이득은 두드러지는데, DAPA-CKD 및 EMPA-KIDENY 임상연구에 참여한 IgA신장병증 환자들에서 콩팥병 진행을 무려 51% 낮추었다(상대위험도 0.49, 95% 신뢰구간 0.32 to 0.74) [15,17,20]. 이러한 결과를 바탕으로 예측 모델을 적용해보면, 비당뇨병 만성콩팥병 환자 1,000명에서 SGLT2억제제를 사용하면 콩팥병 진행이 15명에서 적게 생기고 급성콩팥손상이 5명 덜 발생하는 반면, 케토산증이나 하지 절단의 위험은 발생하지 않는 것으로 나온다[15]. 결국 SGLT2억제제는 당뇨병 여부와 무관하게, 그리고 만성콩팥병의 원인 질환과도 무관하게 콩팥병 진행을 억제시키는 효과를 보여주고 있다. KDIGO 2021 만성콩팥병의 혈압관리에 대한 임상진료지침에서는 알부민뇨가 동반된 비당뇨병 만성콩팥병 G1∼G4단계 환자에서 레닌-안지오텐신계억제제를 사용하도록 권고 혹은 제안하고 있지만[25], 알부민뇨가 정상 범위 내인 만성콩팥병 환자에서의 레닌-안지오텐신계억제제 사용의 근거는 부족한 것이 현실이다. 그에 비해 현재까지 만성콩팥병 환자들을 주 대상으로 하였거나 특히 당뇨병이 동반되지 않은 만성콩팥병 환자들을 대상으로 한 SGLT2억제제 임상연구들의 결과를 바탕으로 하여 제시된 KDIGO 2024 만성콩팥병 평가 및 관리에 대한 임상진료지침에 따르면[26], SGLT2억제제는 알부민뇨 200 mg/g 이상이면서 추정사구체여과율 20 mL/min/1.73 m2 이상인 비당뇨병 만성콩팥병 환자 혹은 알부민뇨 수준과 무관하게 심부전이 동반된 비당뇨병 만성콩팥병 환자에서 사용하도록 권고하고 있다[26]. 또한 알부민뇨 200 mg/g 미만이면서 추정사구체여과율 20∼45 mL/mL/1.73 m2인 비당뇨병 만성콩팥병 환자에서도 SGLT2억제제 사용을 제안하고 있다[26]. 물론, 당뇨병콩팥병에서와 마찬가지로 신대체요법 시작까지 SGLT2억제제를 지속하도록 한다. 결론적으로, 레닌-안지오텐신계억제제가 치료 근거를 가지지 못한 범주인, 알부민뇨가 정상인 만성콩팥병 G3b단계 그리고 G4단계 일부에 해당하는 비당뇨병 만성콩팥병 환자들에서는 SGLT2억제제가 유일하게 콩팥 이득의 근거를 가지고 사용될 수 있다(Fig. 2).
Fig. 2.
Indications for initiating RAS and SGLT2 inhibitors in nondiabetic chronic kidney disease. (A) Range of indications for initiating RAS inhibitors (red-colored boxes), and (B) SGLT2 inhibitors (B, blue-colored boxes) in nondiabetic chronic kidney disease based on the KDIGO GFR and albuminuria categories for staging chronic kidney disease according to KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease [26] are shown. (C) SGLT2 inhibitors may be initiated in patients with nondiabetic chronic kidney disease even with albuminuria < 200 mg/g and eGFR 20∼45 mL/min/1.73 m², as well as in patients with albuminuria ≥ 200 mg/g and eGFR ≥ 20 mL/min/1.73 m², and then continued even if the eGFR falls below 20 mL/min/1.73 m², unless kidney replacement therapy is initiated.
RAS, renin-angiotensin system; SGLT2, sodium glucose cotransporter 2; KDIGO, Kidney Disease: Improving Global Outcomes; GFR, glomerular filtration rate; eGFR, estimated glomerular filtration rate.
3. 고혈압
고혈압은 만성콩팥병의 대표적인 원인 질환 중 하나이면서 콩팥병 진행의 위험인자이기도 하다[24,27]. SGLT2억제제는 항고혈압제로 개발된 것은 아니지만 혈압강하효과가 보고되고 있다. 메타분석 결과에 따르면 2형당뇨병 환자에서 SGLT2억제제를 4∼12주간 사용하면 24시간 활동혈압이 위약 대비 3.61 mm Hg 더 감소하는데, 이는 하이드로클로로싸이아자이드(hydrochlorothiazide) 12.5∼25 mg의 항고혈압 효과와 유사하다[27-29]. 또한, 3개월의 다파글리플로진(dapagliflozin) 투여 관찰 연구에서도 24시간 수축기혈압과 주간 수축기혈압의 유의한 감소가 확인되었다[27,30].
4. 고칼륨혈증
고칼륨혈증은 만성콩팥병 환자 약 2∼35%에서 사구체여과율 수준에 따라 흔히 발생하는 합병증 중 하나이다[27]. 레닌-안지오텐신계억제제를 사용하면서 고칼륨혈증을 유발할 수 있는 조건은 만성콩팥병 외에도 당뇨병, 비보상울혈심부전, 체액 결핍, 고령 등이 있다[23]. 임상진료지침들에서는 레닌-안지오텐신계억제제나 무기질부신피질호르몬수용체대항제(mineralocorticoid receptor antagonist) 투여 후 고칼륨혈증이 발생하더라도 감량이나 중단을 하기보다는 혈청포타슘을 줄이기 위한 조치를 먼저 하도록 권장하고 있다[23-25]. 포타슘 상승을 억제하기 위해서 포타슘결합제 외에도 고리작용이뇨제나 싸이아자이드 등의 이뇨제를 사용할 수 있는데[24,25], 이뇨제의 일종으로 볼 수 있는 SGLT2억제제도 역시 심각한 고칼륨혈증의 위험을 감소시킬 수 있을 뿐 아니라(위험비 0.84, 95% 신뢰구간 0.76 to 0.93) 심혈관위험이 높은 당뇨병 혹은 만성콩팥병 환자에서 고칼륨혈증 발생을 억제할 수 있다[31].
6. 빈혈
건강인과 비교하여 추정사구체여과율 60 mL/min/1.73 m2 미만인 만성콩팥병 환자 남녀 모두에서 평균 헤모글로빈은 감소하며, 이는 사구체여과율이 감소할수록 더욱 떨어지게 된다[34]. Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure (DAPA-HF), Dapagliflozin Effect on Cardiovascular Events-Thrombolysis in Myocardi-al Infarction 58 (DECLARE-TIMI 58) 및 EMPA-REG OUTCOME 결과들로부터[16,35,36], 다파글리플로진 혹은 엠파글리플로진(empagliflozin)은 적혈구용적률(hema-tocrit)을 증가시켜 빈혈을 호전시킨다는 사실이 관찰되었다[37]. SGLT2억제제의 빈혈에 대한 효과는 아마도 이뇨 작용에 따른 혈액농축(hemoconcentration), 적혈구형성호르몬(erythropoietin) 자극에 따른 적혈구 생성 증가, 교감신경과다활동(sympathetic hyperactivity)의 조절 등에 의하여 이루어진다고 추정되고 있으나 정확한 기전은 아직 확인되지 않았다[37]. 빈혈이 만성콩팥병의 진행과 연관되어 있다는 점을 고려하면 SGLT2억제제에 의한 빈혈교정의 효과는 또 다른 장점이 될 수 있겠다.
7. 만성콩팥병에서 SGLT2억제제 사용 시 주의점
SGLT2억제제 사용과 관련하여 일반적인 sick day proto-col, 수술 전후 관리, 발관리 등 외에도 만성콩팥병 환자에서 SGLT2억제제 투여 시 고려해야 할 점이 있다[23,38]. SGLT2억제제 사용 후 초기에 사구체여과율이 감소하는 상황은 비단 SGLT2억제제뿐 아니라 혈류역학 변화를 일으키는 모든 약물들에서도 마찬가지이다. 즉 레닌-안지오텐신계억제제, 무기질부신피질호르몬수용체대항제, 이뇨제 및 기타 항고혈압제들도 마찬가지로 사구체여과율 저하를 유발한다[38]. 사구체여과율에 영향을 줄 수 있는 약물들의 특성을 고려하여 신장학 분야 임상진료지침들에서는 층상화접근법(layered approach)을 제안하고 있다[23,38]. 즉, 다른 분야에서는 기둥접근법(pillar approach), 예를 들어 당뇨병콩팥병 예방과 치료를 위하여 혈당조절, 생활습관교정, 레닌-안지오텐신계억제제, SGLT2억제제, 비스테로이드부신피질호르몬수용체대항제(non-steroidal mineralocorticoid receptor antagonist) 등을 각 기둥으로 설정하여 신전을 세우는 모습으로 질환 치료의 모델을 제시하고 있는 반면[39,40], 신장학 분야에서는 각 혈류역학 변화를 일으키는 약물들은 아무리 일차선택약물이라 하더라도 한꺼번에 투여하는 것이 아닌 순차적으로 시작하는 것이 필요하다고 강조하고 있다[38]. 새로운 약물은 한 번에 하나씩 투여하고 그 반응과 잔여 위험을 재분석하는, 끊임없는 재평가가 필요한 것이며[38], 이것이 만성콩팥병 환자 치료에서 층상화접근법이 더 타당한 이유가 된다. 예를 들어, 만성콩팥병 환자에서 레닌-안지오텐신계억제제 투여 2∼4주 후 혈청포타슘이나 크레아티닌 수준이 감내할 수 있는 변화만 있다면 이어서 SGLT2억제제 투여를 시작하고 추적검사에서 추정사구체여과율의 감소가 30% 이내라면 중단하지 않고 사용하도록 한다[23,24]. 또한 레닌-안지오텐신계억제제와 달리 콩팥 혹은 심혈관위험 감소를 위해 투여되는 SGLT2억제제는 시작 용량과 유지 용량이 같고 사구체여과율 수준에 따른 투여량 적정(dose titration)이 필요 없다는 점도 명심할 필요가 있다[14].
결론
지난 수십여 년 동안 수많은 노력으로 여러 나라에서의 만성콩팥병 유병률은 비교적 안정적인 추이를 보이고 있다. 그러나 우리나라의 경우 인구 노령화가 유난히 빠르고 또한 당뇨병 유병자 수가 지속적으로 증가 추세인 점 등을 고려하면 향후에도 우리나라의 만성콩팥병 환자의 절대 수는 크게 증가할 것이다[13,24]. 기존의 레닌-안지오텐신계억제제가 수십여 년 동안 만성콩팥병 치료에 있어 지대한 공헌을 해온 것은 맞지만 한계가 있었다. 이제는 만성콩팥병 치료의 또 다른 근간이 된 SGLT2억제제가 만성콩팥병 환자의 경과를 크게 바꿀 수 있을 것으로 기대된다. 안타깝게도 우리나라에서는 만성콩팥병 치료에 대한 적응증을 가지고 있는 오리지널 다파글리플로진의 철수가 예정되어 있다는 소식이 있다. 만성콩팥병과 그 결과인 말기콩팥병으로 지출되는 막대한 의료 비용을 고려해 볼 때[24], 만성콩팥병 치료 약물의 선택은 폭넓게 유지될 필요가 있다.
SGLT2억제제 외에 우리나라에서도 이제 출시된 비스테로이드무기질부신피질호르몬수용체대항제, 그리고 차세대 만성콩팥병 치료제로 기대되는 글루카곤유사펩타이드-1수용체작용제(glucagon-like peptide-1 receptor agonist) 등도 향후 만성콩팥병 치료에 끼칠 영향력이 무척 기대되고 있다[41,42]. 덕택에 만성콩팥병과 맞서 싸울 무기가 많아진다면 만성콩팥병 환자들의 예후는 우리가 기대한 것 이상으로 많이 달라질 것이다. 물론 SGLT2억제제 등이 의료보건에 끼치는 영향은 향후 10∼15년 이후에나 뚜렷하게 나타날 것이므로 인내심이 필요할 수 있다[43]. 그러나 지금까지 나온 근거에 기반하면, 알부민뇨 수준과는 무관하게 추정사구체여과율 20 mL/min/1.73 m2 이상인 모든 2형당뇨병 콩팥병 환자와 알부민뇨 200 mg/g 미만이면서 추정사구체여과율 45 mL/min/1.73 m2 이상인 경우를 제외한 모든 비당뇨병 만성콩팥병 환자에서는 지금이라도 SGLT2억제제를 시작하여 신대체요법 전까지 지속해야 할 것이다. SGLT2억제제의 뛰어난 콩팥과 심혈관이득을 고려한다면 이제는 거의 모든 만성콩팥병 환자에서 SGLT2억제제의 사용은 필수적이므로 더 이상 주저하거나 지체할 필요가 없다.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




