2021 당뇨병 진료지침: 약물치료 및 Korean Diabetes Association Support System
2021 Clinical Practice Guidelines for Diabetes: Pharmacotherapy and the Korean Diabetes Association Support System
Article information
Trans Abstract
The most important change introduced in the pharmacotherapy session for the 2021 Clinical Practice Guidelines for Diabetes is the recommendation of two different strategies according to the patient's condition. One approach is to optimize the blood glucose levels, while the other approach is to reduce adverse cardiovascular events or mortality, especially in patients with comorbidities (e.g., heart failure, atherosclerotic cardiovascular disease, or chronic kidney disease). We suggest four algorithms that take into account the patient's condition (algorithms 1 to 4). The Korean Diabetes Association (KDA) developed a web-based clinical decision support system, known as the KDA support system (KDASS), which helps with the diagnosis of diabetes or gestational diabetes and whether to use glucose-lowering agents according to the patient's condition.
서론
이번 2021년 당뇨병 진료지침의 가장 큰 개정사항은 당뇨병 약물 선택 시 혈당조절을 중심으로 접근하는 경우와 동반질환을 중심으로 접근해야 하는 경우로 나눈 것이다[1]. 알고리듬을 4가지로 나누었는데 당뇨병 치료 시작(Fig. 1), 병용요법(Fig. 2), 주사제 포함한 치료(Fig. 3), 그리고 심부전, 죽상경화심혈관질환 혹은 만성신장질환 등 동반질환이 있는 경우(Fig. 4)로 나누어서 제시하였다. 약물 선택 시 환자의 상태에 따라 고려할 사항도 많은데 당뇨병 약물은 기전에 따라 계열의 종류만 9가지이고 또 계열마다 많은 개별 약물들이 존재하며 또 약물마다 병용기준의 허가 사항이나 급여 기준이 달라서 진료현장에서 고충이 상당히 크다. 진료지침에 근거한 당뇨병 진단 및 치료약물 결정을 진료현장에서 좀 더 쉽게 적용할 수 있도록 돕기 위하여 대한당뇨병학회 주도하에 최초로 진료지침에 근거한 온라인 기반 임상결정 보조수단을 개발하였기에 간단히 소개하고자 한다.
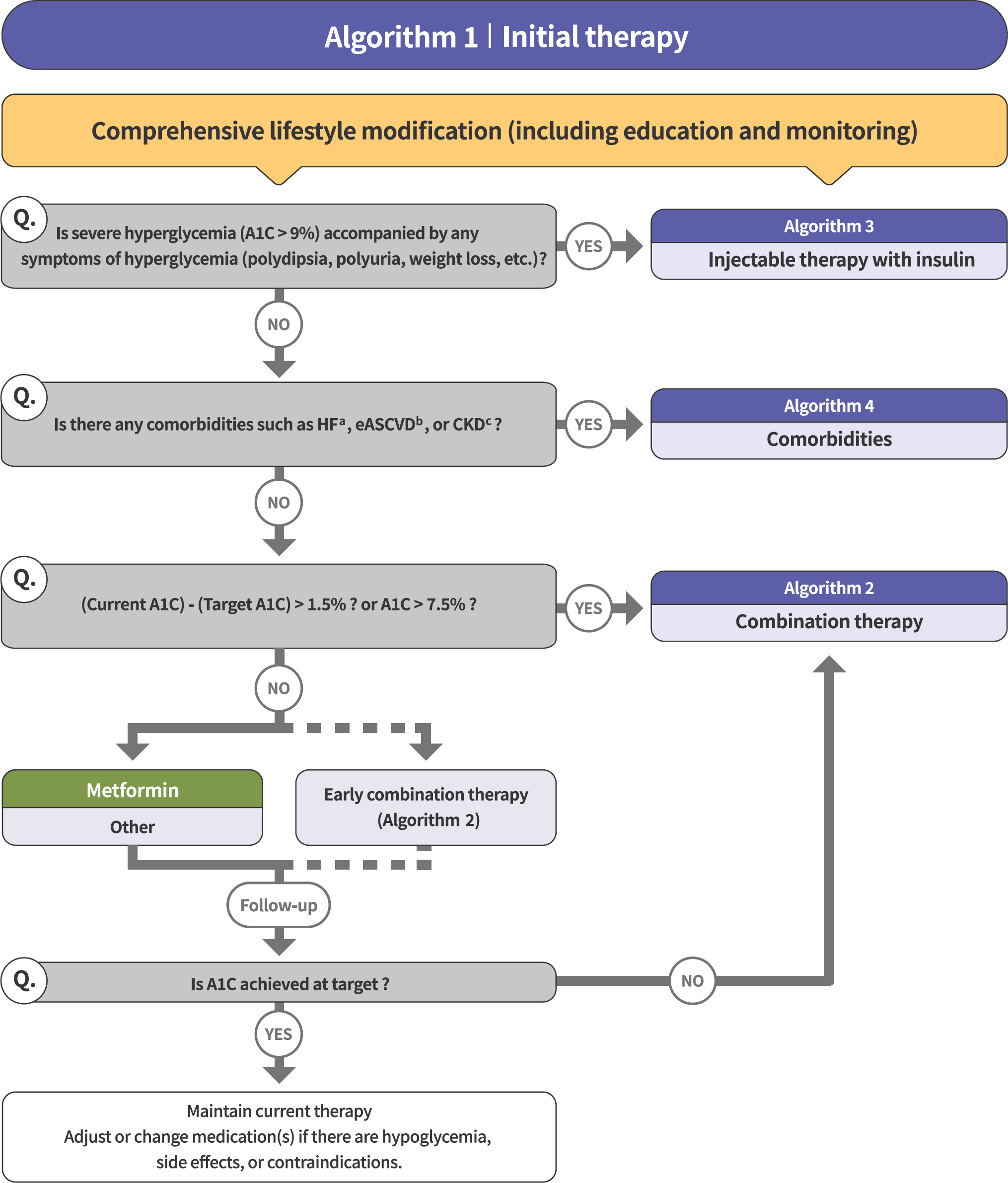
Treatment algorithm 1 (initial therapy) for patients with type 2 diabetes mellitus (T2DM). The algorithm strat-ifies the strategy of glycemic control for T2DM based on initial glycosylated hemoglobin (A1C) levels and underlying comorbidities. For newly diagnosed T2DM, begin with comprehensive lifestyle modification (LSM) at the time of diagnosis and monitor continuously. If the initial severe hyperglycemia (A1C level > 9.0%) is accompanied by symptoms of hyperglycemia (polydipsia, polyuria, weight loss, etc.), insulin treatment should be prioritized (algorithm 3). If heart failure (HF), established atherosclerotic cardiovascular disease (eASCVD), or chronic kidney disease (CKD) are present, follow algorithm 4. If glycemic target is not achieved within 3 months after LSM, then glucose-lowering agent should be initiated promptly. If the current A1C is 1.5% higher than that of the target A1C or the current A1C level is > 7.5%, follow algorithm 2 (combination therapy). If the A1C level is 7.5% or less, metformin monotherapy is recommended as a first-line therapy. However, if there are contraindications or intolerable side effects related to metformin use, a different class of medications can be considered. Instead of metformin monotherapy, early combination therapy could be considered to reduce the risk of failure of glycemic control in some patients with newly diagnosed T2DM.
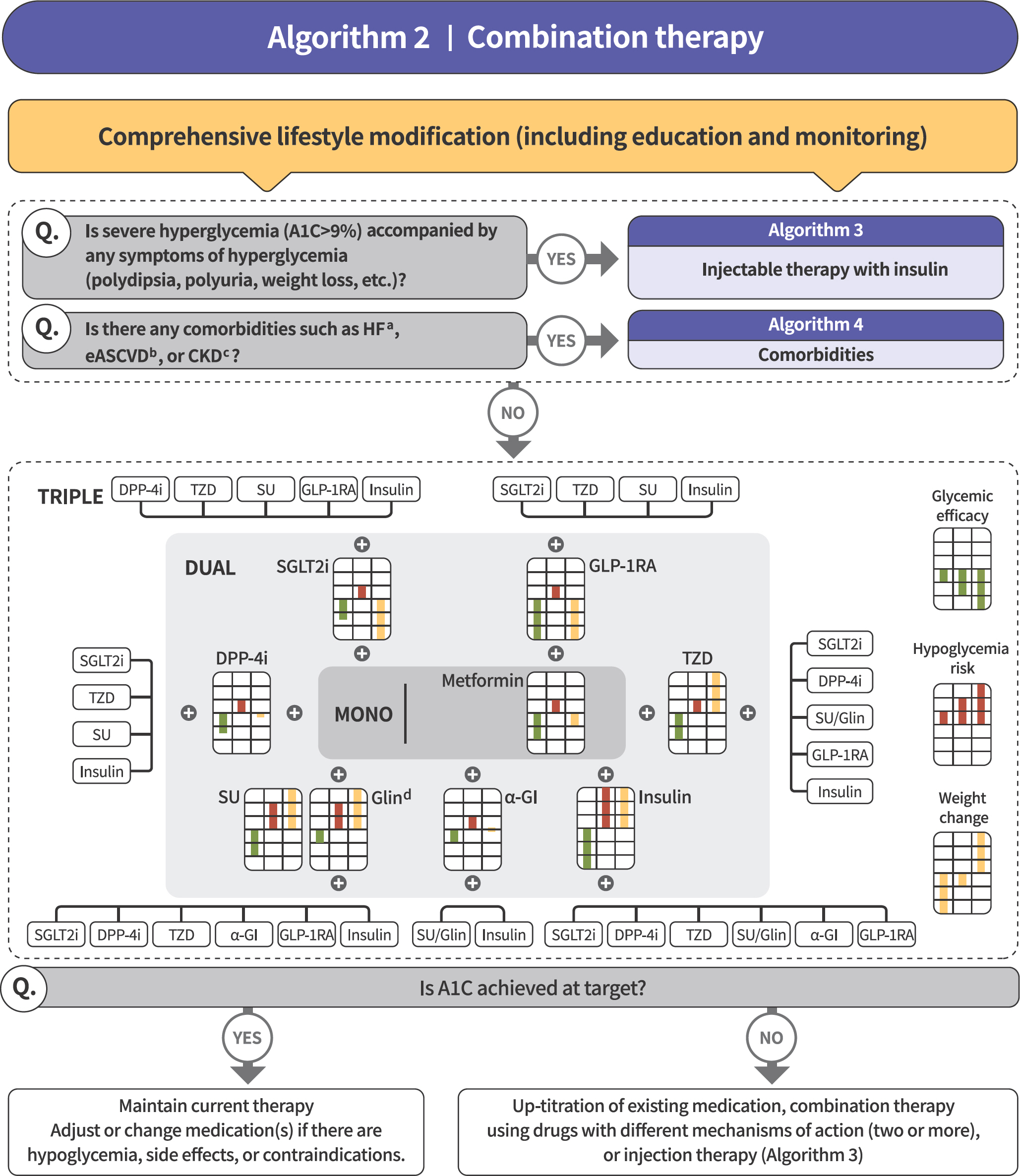
Treatment algorithm 2 (combination therapy) for patients with type 2 diabetes mellitus (T2DM). If the current glycosylated hemoglobin (A1C) is 1.5% higher than that of the target A1C or the current A1C level is > 7.5%, combination therapy is recommended. If the target A1C level has not been achieved, the up-titration of existing medication, combination therapy using medications with different mechanisms of action, or use of injectable medication should actively be considered as soon as possible. When choosing glucose-lowering agents, consider glucose-lowering efficacy, hypoglycemia risk or weight change, side effects, treatment acceptability, age, personal value of life, and cost. The characteristics of glucose-lowering agents are expressed as a bar scale. Each color shows glycemic efficacy (green), hypoglycemia risk (red), and body weight change (yellow).
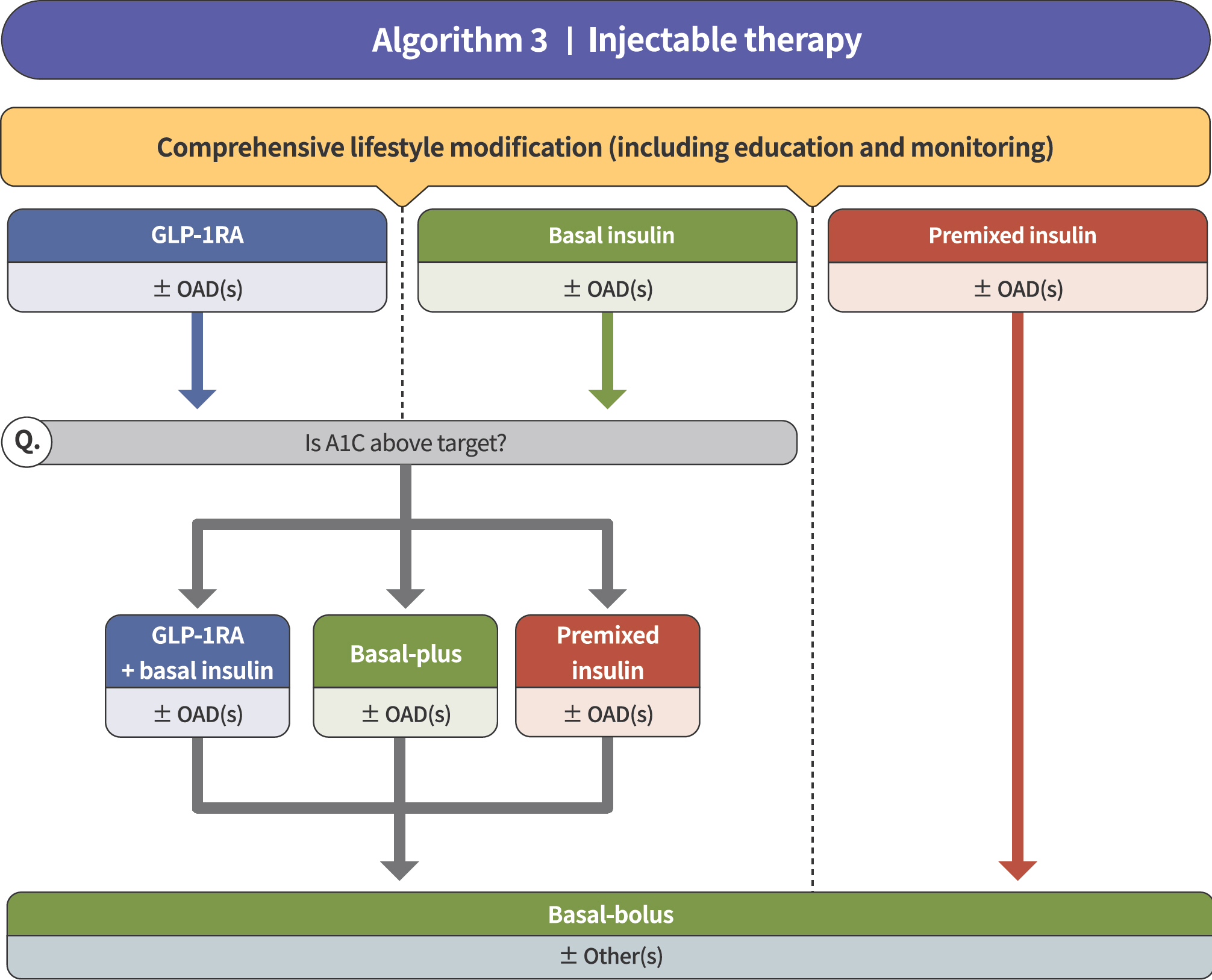
Treatment algorithm 3 (injectable therapy) for patients with type 2 diabetes mellitus (T2DM). If the glycosylated hemoglobin (A1C) level is > 9.0% and symptomatic hyperglycemia or metabolic decompensation is present, insulin therapy can be initiated with or without oral anti-diabetic drug (OAD) in patients with T2DM. Injectable therapy (glucagon-like peptide-1 receptor agonist [GLP-1RA] or insulin) is recommended when potent glucose-lowering efficacy is required. The addition of GLP-1RA, basal insulin, or premixed insulin is recommended equally. If A1C target is not achieved with GLP-1RA or basal insulin-based therapy, free or fixed-ratio combination therapy of GLP-1RA and basal insulin could be considered. Intensification of insulin therapy with premixed insulin twice daily, basal-plus, or basal-bolus is also recommended to enhance blood glucose control.
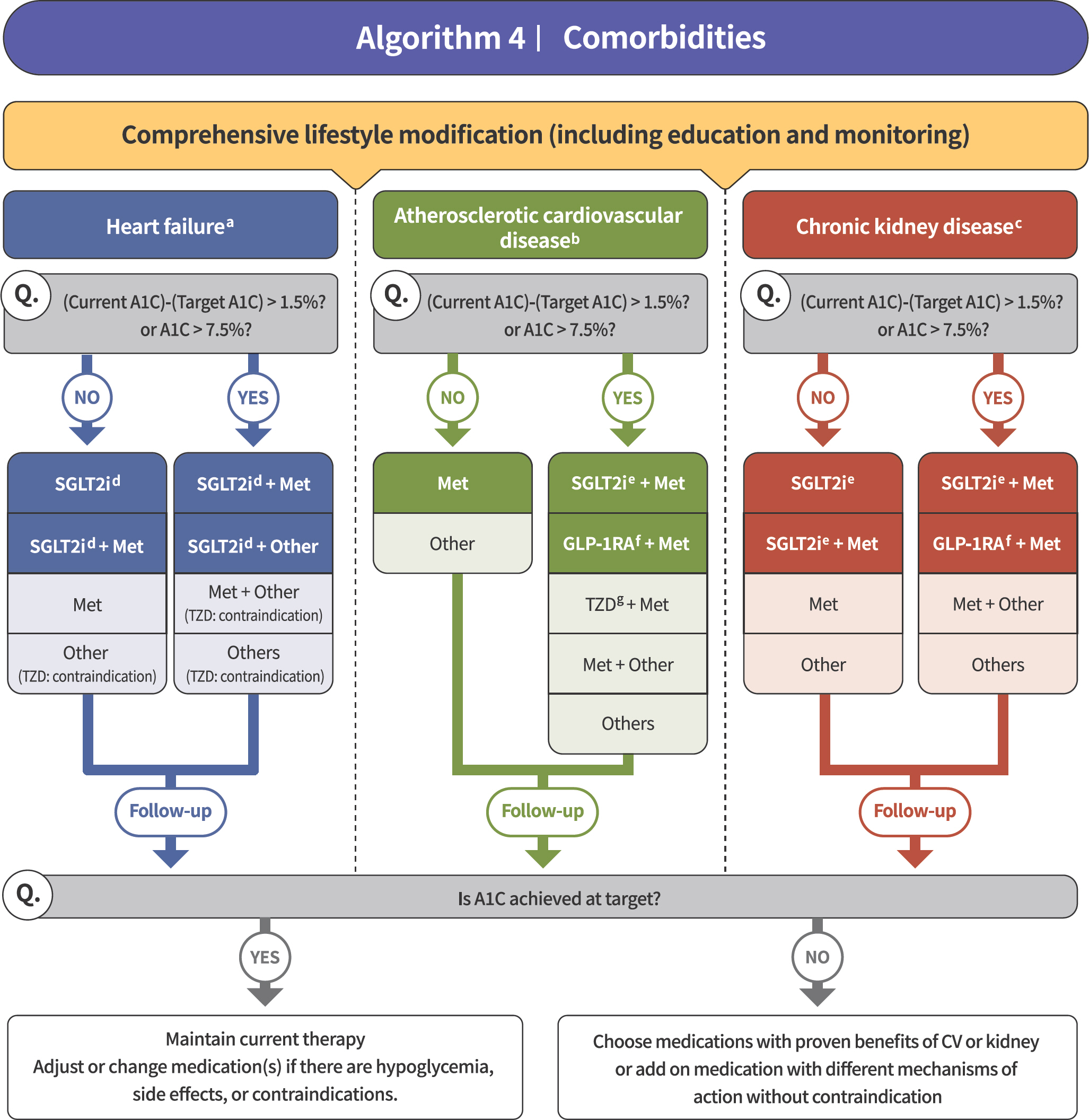
Treatment algorithm 4 (comorbidities) for patients with type 2 diabetes mellitus who have heart failure (HF), established atherosclerotic cardiovascular disease (eASCVD), or chronic kidney disease (CKD). If patients have underlying above comorbidities, glucose-lowering agents, including sodium-glucose cotransporter 2 (SGLT2) inhibitor or gluca-gon-like peptide-1 receptor agonist (GLP1-RA), are the preferred choice. For patients with HF, glucose-lowering agents, including SGLT2 inhibitors with proven cardiovascular (CV) benefits, should be prioritized. Regimens that include SGLT2 inhibitors or GLP-1RAs with proven CV benefits should be prioritized for combination therapy in patients with eASCVD. For patients with albuminuria or reduced estimated glomerular filtration rate (eGFR), glucose-lowering agents, including SGLT2 inhibitors with proven renal and CV benefits, should be prioritized.
당뇨병성인에서 혈당조절 목표
혈당을 왜 열심히, 적극적으로 조절해야 하는가? 그것은 미세혈관 및 대혈관합병증을 예방하기 위해서이다[무작위대조연구, 일반적권고] [2].
그렇다면 혈당을 어디까지 조절해야 하며 기준은 무엇인가? 2형당뇨병 성인에게서 일반적인 혈당조절 목표는 당화혈색소 6.5% 미만이고[무작위연구, 일반적권고] 1형당뇨병 성인에게서 일반적인 혈당조절 목표는 당화혈색소 7.0% 미만이다[무작위대조연구, 일반적권고]. 그러나 이것은 일반적인 조절 목표이고 환자의 신체적, 정신적, 사회적 여건, 기대여명, 동반질환의 중증도 혹은 저혈당 위험도에 따라 개별화한다[비무작위대조연구, 일반적권고].
2형당뇨병의약물치료
이번 진료지침의 가장 큰 핵심이자 변화는 2형당뇨병의 약물치료를 크게 혈당조절을 중심으로 약물을 선택해야 하는 경우와 동반질환을 고려하여 약물을 선택해야 하는 경우로명확히 나누어서 접근하도록 명시하였다는 것이다. 최근에 심혈관질환이 동반된 경우에 특정 약제들의 유익을 입증한 약제들이 나와서 마치 모든 당뇨병 환자에서 무조건 다 이러한 약제들을 먼저 써야하는 것처럼 정보를 잘못 인지하고 있는 경우가 많아서 진료 현장에서 혼선이 있다. 지금까지의 임상연구결과들을 바탕으로 환자에 따라 혈당조절 위주로 약제를 선택할 것인지 아니면 동반질환이 있는 경우 이를 고려하여 약제를 선택할 것인지를 나누어서 권고하였다. 그래서 알고리듬을 다음과 같이 4가지로 나누어서 제시하였다.
1. 당뇨병 치료 시작(알고리듬 1)
모든 당뇨병 치료에서 생활습관교정은 언제나 중요하다. 당뇨병 진단 즉시 생활습관교정을 적극적으로 교육하고 지속하도록 모니터링한다[무작위대조연구, 일반적권고].
초진이건 재진이건 간에 심각한 고혈당(당화혈색소 > 9.0%)과 함께 고혈당으로 인한 증상(다음, 다뇨, 체중감소 등)이 동반된 경우는 인슐린 치료를 우선 고려해야 한다[전문가의견, 일반적권고] [3] (Fig. 3).
만일 심부전, 죽상경화심혈관질환, 만성신장질환이 동반되어 있다면 이 질환에서 심혈관이익이 입증된 약제를 포함한 치료를 우선 고려한다[무작위대조연구, 제한적권고] (Fig. 4).
위의 사항들을 점검하여 알고리듬 3이나 4로 가야 하는 경우들이 배제가 되었다면 이제는 고전적으로 해오던 혈당조절 측면에서 접근하면 된다.
약물치료를 시작할 때 목표와 현재 당화혈색소를 고려하여 단독 또는 병용요법을 한다[무작위대조연구, 일반적권고] (Fig. 1). 목표 당화혈색소와 현재 당화혈색소 차이가 1.5%를 초과하거나 처음부터 당화혈색소가 7.5%를 초과하는 경우는 병용요법을 고려하고 그렇지 않으면 단독요법을 고려한다.
약물치료 시 메트포민을 우선 사용하고 금기나 부작용이 없는 한 유지한다[무작위대조연구, 일반적권고]. 그러나 메트포민의 금기나 부작용이 있는 경우에는 다른 계열의 약물을 사용한다[전문가의견, 일반적권고] [4]. 혈당조절 실패의 위험을 낮추기 위해 진단 초기부터 병용요법을 적극적으로 고려한다[무작위대조연구, 일반적권고] (Fig. 2).
2. 병용요법(알고리듬 2)
목표 당화혈색소에 도달하지 못한 경우 기존 약물의 증량 또는 다른 계열 약물과의 병용요법(2제 이상)을 조속히 시행한다(단, DPP-4 [dipeptidyl peptidase]억제제와 GLP-1 [glucagon-like peptide-1]수용체작용제는 병용하지 않는다) [무작위대조연구, 일반적권고] (Fig. 2).
약물 선택 시 혈당강하 효과, 저혈당 위험도, 부작용, 동반질환(심부전, 죽상경화심혈관질환, 만성신장질환) 여부, 치료 수용성, 나이, 환자가 추구하는 삶의 가치, 비용을 고려한다[전문가의견, 일반적권고]. 여기서 각 약제 계열마다 혈당강하 효과(초록)와 저혈당 위험도(빨강), 체중에 미치는 효과(노랑)를 직관적으로 알아볼 수 있도록 막대 그래프로 표시하였다.
약물치료 시 주기적으로 복약순응도를 확인하고, 필요한 경우 약물을 조정한다[전문가의견, 일반적권고].
3. 주사제 포함한 치료(알고리듬 3)
앞서 언급한 것처럼 초진이건 재진이건 간에 심각한 고혈당(당화혈색소 > 9.0%)과 함께 고혈당으로 인한 증상(다음, 다뇨, 체중감소 등)이 동반된 경우는 인슐린 치료를 우선 고려해야 한다[전문가의견, 일반적권고] (Fig. 3).
또한 강력한 혈당강하 효과를 중점적으로 고려할 경우 주사제를 포함한 치료를 우선한다[무작위대조연구, 일반적권고] [4]. 과거의 진료지침에서는 경구약물 실패 시 주사제를 고려하라는 방향이었다면 이번에 개정된 진료지침에서는 어느 단계든지 적극적이고 강력한 혈당조절이 필요할 경우 인슐린이나 GLP-1수용체작용제 등의 주사제를 고려하도록 권고한다.
주사제 치료 시 인슐린이나 GLP-1수용체작용제 중 한 가지만 포함하여 치료를 할 수도 있고 그것으로 혈당조절 목표에 도달하지 못하였을 경우 혈당조절 강화를 위해 GLP-1수용체작용제와 기저인슐린을 병용할 수 있다[무작위대조연구, 제한적권고]. 이 경우 단독제나 고정비율복합제를 고려할 수 있다. 또한 혈당조절 강화를 위해 다회인슐린주사요법을 고려한다[무작위대조연구, 제한적권고].
Korean Diabetes Association Support System: 온라인 기반의 임상결정 보조수단
앞서 언급한 바와 같이, 당뇨병 약물은 그 계열만해도 9가지이고 또 각 계열별로 상당히 많은 개별 약물들이 있으며, 또 개별 약물들 간에 약물작용 시간이나 적응증의 차이가 있는 경우도 있다. 게다가 약물별로 병용요법에 대한 허가사항 및 급여 기준까지 다르기도 하고 또 이 기준마저도 짧은 주기로 계속 업데이트가 되고 있다. 이처럼 당뇨병 약물을 결정할 때 확인하고 고려해야 할 사항들이 너무 많다 보니 실제 진료현장에서 혼선과 고충이 상당히 크다.
약물 선택에서의 고충뿐만 아니라 당뇨병의 진단, 특히 임신당뇨병 진단의 경우에는 포도당내성검사를 시행해도 그 진단기준을 늘 다 기억하고 있기는 어렵다. 따라서 아무리 학회에서 진료지침을 잘 만들고 업데이트를 하여도 그 권고하는 내용들이 실제 진료현장에서 쉽고 빠르게 반영되지 못한다면 무용지물일 것이다. 그래서 대한당뇨병학회에서는 정기적으로 업데이트되는 당뇨병 진료지침의 내용들을 실제 진료현장에서 쉽고 빠르게 적용하는 것을 돕기 위해 학회 주도로는 최초로 온라인 기반의 임상결정 보조수단(clinical decision support system)을 개발하였고, Korean Diabetes Association Support System (KDASS)이라고 명명하였다.
KDASS는 환자 상태에 관한 몇 가지 필수 정보를 입력하여 당뇨병 진단, 임신당뇨병 진단, 초진 약물 선택, 약물병용 허가사항이나 급여 여부를 판단하는 보조수단으로 활용할 수 있다. 현재 대한당뇨병학회 홈페이지에 게시되어 있으며 스마트 폰에서도 사용 가능하다.
결론
2021 당뇨병 진료지침 약물치료 부분에서 가장 중요한 변화는 혈당조절을 중심으로 접근하는 경우와 동반질환이 있을 때 접근하는 경우를 나누어서 제시한 점이다. 그리고 혈당조절을 중심으로 접근하는 것에서 강조된 것은 더 빨리, 더 철저히 혈당조절을 하기 위해 경구약제뿐만 아니라 주사제를 포함한 치료를 적극 활용하라는 것이다. 또 진료지침의 임상활용도를 높이기 위한 학회의 노력이 반영되었다. 요약본에 여러 가지 유용한 부록을 수록하였고, 특히 온라인 기반의 임상결정 보조수단인 KDASS를 학회에서 최초로 개발하였는데, 진료현장에서 당뇨병, 임신당뇨병을 진단하거나 환자 상태에 따라 어떤 약물을 쓰는 것이 좋을지 추천을 받고자 할 때, 또 병합요법의 허가, 급여사항을 확인하는 데 도움이 될 것으로 기대한다.