

ņä£ļĪĀ
ļ©ĖņŗĀļ¤¼ļŗØ(machine learning, ML)ņØĆ ņĄ£ĻĘ╝ ļ│æņøÉ ņ×ÉļŻīņØś ņĀäņé░ĒÖö, ņ×äņāüņ×ÉļŻī ļłäņĀü, ļīĆĻĘ£ļ¬© ņ×ÉļŻīļź╝ ņ▓śļ”¼ĒĢĀ ņłś ņ׳ļŖö ņ╗┤Ēō©Ēä░ņØś ņĀĆņן ļ░Å Ļ│äņé░ļŖźļĀźņØś ņ”ØĻ░ĆņÖĆ ĒĢ©Ļ╗ś ļ¦ÄņØĆ Ļ┤Ćņŗ¼ņØä ļ░øņ£╝ļ®░ ņŚ¼ļ¤¼ ņ×äņāü ļČäņĢ╝ ņŚ░ĻĄ¼ņÖĆ ņ¦äļŻīņŚÉņä£ ĒÖ£ņÜ®ļÉśĻ│Ā ņ׳ļŗż. ļŗ╣ļć©ļ│æĻ│╝ ļé┤ļČäļ╣äņ¦łĒÖś ļČäņĢ╝ņŚÉņä£, ļ©ĖņŗĀļ¤¼ļŗØĻ│╝ ņŚ░Ļ┤ĆļÉśņ¢┤ Ļ▓īņ×¼ļÉ£ ļģ╝ļ¼ĖņØś ņłśļŖö PubMed Ļ▓ĆņāēĻĖ░ņżĆ 1986ļģäļČĆĒä░ 2020ļģä 1ņøöĻ╣īņ¦Ć ņĢĮ 2,000Ļ▒┤ņŚÉ ļŗ¼ĒĢśļ®░, ņĄ£ĻĘ╝ 10ļģäĻ░ä ĻĖ░ĒĢśĻĖēņłśņĀüņØĖ ņ”ØĻ░ĆņČöņäĖļź╝ ļ│┤ņØ┤Ļ│Ā ņ׳ļŗż. ļ│Ė ņóģņäżņŚÉņä£ļŖö ļ©ĖņŗĀļ¤¼ļŗØĻ│╝ ņŚ░Ļ┤ĆļÉ£ ņŚ¼ļ¤¼ Ļ░£ļģÉņŚÉ ļīĆĒĢ£ Ļ░äļץĒĢ£ ņĀĢņØś, ļŗ╣ļć©ļ│æĻ│╝ ļé┤ļČäļ╣äņ¦łĒÖśņŚÉņä£ ļ©ĖņŗĀļ¤¼ļŗØņØä ĒÖ£ņÜ®ĒĢ£ ņśłņŗ£ ņŚ░ĻĄ¼ļōżņØä ņé┤ĒÄ┤ļ│┤Ļ│Ā, ņČöĒøä ļŗ╣ļć©ļ│æ ļ░Å ļé┤ļČäļ╣äņ¦łĒÖś ņ×äņāüņŚ░ĻĄ¼ņÖĆ ņ¦äļŻīņŚÉ ņ׳ņ¢┤ ļ©ĖņŗĀļ¤¼ļŗØņØś ĒÖ£ņÜ®ļ░®ņĢł ļ░Å ļ░£ņĀäĻ░ĆļŖźņä▒ņŚÉ ļīĆĒĢ┤ ļģ╝ņØśĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ļ©ĖņŗĀļ¤¼ļŗØ: Ļ░£ļģÉ ņåīĻ░£
1. ņØĖĻ│Ąņ¦ĆļŖź, ļ©ĖņŗĀļ¤¼ļŗØ, ĻĘĖļ”¼Ļ│Ā ļöźļ¤¼ļŗØ
ņØĖĻ│Ąņ¦ĆļŖź(artificial intelligence, AI), ļ©ĖņŗĀļ¤¼ļŗØ(ML), ļöźļ¤¼ļŗØ(deep learning)ņØĆ ņØśĒĢÖ ļČäņĢ╝ņŚÉņä£ ļ¦ÄņØĆ Ļ▓ĮņÜ░ ļÅÖņŗ£ņŚÉ ņé¼ņÜ®ļÉśĻ▒░ļéś Ļ░ÖņØĆ ņØśļ»ĖļĪ£ Ēś╝ņÜ®ļÉśĻ│Ā ņ׳ļŗż. ļ»ĖĻĄŁņŗØĒÆłņØśņĢĮĻĄŁ(U.S. Food and Drug Administration)ņØĆ ņØĖĻ│Ąņ¦ĆļŖźņØä ņĪ┤ļ¦źņ╗żņŗ£ņØś ņĀĢņØśņŚÉ ļö░ļØ╝ ŌĆśņ¦ĆļŖźņØ┤ ņ׳ļŖö ĻĖ░Ļ│äļź╝ ļ¦īļō£ļŖö Ļ│╝ĒĢÖĻ│╝ Ļ│ĄĒĢÖ(the science and engineering of making intelligent machines, especially intelligent computer programs)ŌĆÖņ£╝ļĪ£ ņĀĢņØśĒĢśņśĆļŗż[1,2]. ņØ╝ļ░śņĀüņ£╝ļĪ£ ņ¦ĆļŖźņØĆ ņ×ÉĻĖ░ņØĖņŗØ, Ļ▓ĮĒŚśņĀü ņ¦ĆņŗØ ļō▒ ĒżĻ┤äņĀüņØĖ ņśüņŚŁņØä ņ¦Ćņ╣ŁĒĢśļŖö Ļ░£ļģÉņØ┤ņ¦Ćļ¦ī, ĻĘĖ ņżæ ĒĢÖņŖĄĻ│╝ ņČöļĪĀņØĆ Ēśä ņŗ£ņĀÉņŚÉņä£ ņØĖĻ│Ąņ¦ĆļŖźņØä ņĀĢņØśĒĢśļŖö Ļ░Ćņן ņżæņÜöĒĢ£ ņÜöņåīļĪ£ ņØĖņ¦ĆļÉśĻ│Ā ņ׳ļŗż[1]. ņØĖĻ│Ąņ¦ĆļŖźņØ┤ Ļ░Ćņן ĒżĻ┤äņĀüņØĖ ņāüņ£ä Ļ░£ļģÉņØ┤ļØ╝ļ®┤, ļ©ĖņŗĀļ¤¼ļŗØņØĆ ŌĆśļŹ░ņØ┤Ēä░ļĪ£ļČĆĒä░ ņŖżņŖżļĪ£ ĒĢÖņŖĄĒĢśņŚ¼ ļČäļźśļéś ņśłņĖĪ ļō▒ņØś ņłśĒ¢ēļŖźļĀźņØä Ļ░£ņäĀĒĢĀ ņłś ņ׳ļŖö ņåīĒöäĒŖĖņø©ņ¢┤ļéś ņĢīĻ│Āļ”¼ņ”śņØä ļööņ×ÉņØĖŌĆÖĒĢśĻĖ░ ņ£äĒĢ£ ņØĖĻ│Ąņ¦ĆļŖźņØś ĒĢ£ ļČäņĢ╝ļĪ£ ņĀĢņØśļÉĀ ņłś ņ׳ļŗż. ļö░ļØ╝ņä£ ļ©ĖņŗĀļ¤¼ļŗØņØĆ ņØĖĻ│Ąņ¦ĆļŖźņŚÉ ĒżĒĢ©ļÉśļŖö Ļ░£ļģÉņØ┤ļéś, ņØĖĻ│Ąņ¦ĆļŖźņØ┤ Ļ╝Ł ļ©ĖņŗĀļ¤¼ļŗØņØä ņ¦Ćņ╣ŁĒĢśļŖö Ļ▓āņØĆ ņĢäļŗłļŗż. ļöźļ¤¼ļŗØ Ēś╣ņØĆ ņŗ¼ņĖĄņŗĀĻ▓Įļ¦Ø(deep neural network)ņØĆ ļ©ĖņŗĀļ¤¼ļŗØņØś ĒĢ£ ņóģļźśļĪ£, ņŚ¼ļ¤¼ Ļ▓╣ņØś ņŗĀĻ▓Įļ¦ØņØä ņīōņĢä ņé¼ļ×īņØś ļæÉļćīņÖĆ ņ£Āņé¼ĒĢśĻ▓ī ņäżĻ│äĒĢ£ ņĢīĻ│Āļ”¼ņ”śņØä ņ¦Ćņ╣ŁĒĢ£ļŗż. 2018ļģä Ļ░£ņĄ£ļÉ£ 3ņ░© ML for Health workshopņŚÉ ļö░ļź┤ļ®┤, ņĀäĒåĄņĀüņØĖ Ļ│ĄĒĢÖļČäņĢ╝ ņŚöņ¦Ćļŗłņ¢┤ ļ░Å ņŚ░ĻĄ¼ņ×ÉļōżņØĆ ļ│ĖņØĖļōżņØś ņŚ░ĻĄ¼ļČäņĢ╝ļź╝ ņ¦Ćņ╣ŁĒĢĀ ļĢī ļ©ĖņŗĀļ¤¼ļŗØņØ┤ļØ╝ļŖö ļŗ©ņ¢┤ļź╝ ļŹö ņäĀĒśĖĒĢśņśĆņ£╝ļéś, ņ×äņāüņØśņé¼ļōżņØĆ ļŹö ļäōņØĆ ņØśļ»ĖņØś ņØĖĻ│Ąņ¦ĆļŖźņØ┤ļØ╝ļŖö ļŗ©ņ¢┤ļź╝ ĒØöĒ׳ ĒÖ£ņÜ®ĒĢśņśĆļŗż. ņŚ░ĻĄ¼ ņ╗żļ«żļŗłĒŗ░ Ļ░ä ņÜ®ņ¢┤ĒÖ£ņÜ® ņ░©ņØ┤ļŖö ņåīĒåĄ ņןņĢĀ ļ░Å ļČłĒĢäņÜöĒĢ£ ņśżļźśļź╝ ņ£Āļ░£ĒĢĀ Ļ░ĆļŖźņä▒ņØ┤ ņ׳ņ¢┤, ļ©ĖņŗĀļ¤¼ļŗØ Ļ┤ĆļĀ© ņÜ®ņ¢┤ņØś ņĀĢĒÖĢĒĢ£ ņĀĢņØś ļ░Å ņé¼ņÜ®ņŚÉ ļīĆĒĢ£ Ļ│ĄĒåĄņØś ļģ╝ņØśĻ░Ć ņČöĒøä ĒĢäņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż[3].
2. ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śĻ│╝ ĒÅēĻ░Ćņ¦ĆĒæ£
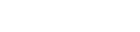
ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śņØĆ Ēü¼Ļ▓ī ņ¦ĆļÅäĒĢÖņŖĄ(supervised learning), ļ╣äņ¦ĆļÅäĒĢÖņŖĄ(unsupervised learning), ņżĆņ¦ĆļÅäĒĢÖņŖĄ(semi-supervised learning), Ļ░ĢĒÖöĒĢÖņŖĄ(reinforcement learning) 4Ļ░Ćņ¦Ć ļ▓öņŻ╝ļĪ£ ļéśļłäņ¢┤ ļ│╝ ņłś ņ׳ļŗż(Table 1) [4-7]. ņ¦ĆļÅäĒĢÖņŖĄņØĆ ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śņØä ĒĢÖņŖĄņŗ£ĒéżĻĖ░ ņ£äĒĢ┤ ļŹ░ņØ┤Ēä░ņÖĆ ņĀĢļŗĄņ¦Ć(ļĀłņØ┤ļĖö, label)ļź╝ ĒĢ©Ļ╗ś ĒĢäņÜöļĪ£ ĒĢ£ļŗż. ņ¦ĆļÅäĒĢÖņŖĄņØś ļ¬®Ēæ£ļŖö ĻĖ░ņĪ┤ ļŹ░ņØ┤Ēä░ņÖĆ ļĀłņØ┤ļĖöĻ│╝ņØś Ļ┤ĆĻ│äļź╝ ļ░öĒāĢņ£╝ļĪ£, ņāłļĪ£ņÜ┤ ļŹ░ņØ┤Ēä░Ļ░Ć ļōżņ¢┤ņÖöņØä ļĢī ĻĖ░ņĪ┤ ņ×ÉļŻīņŚÉ ļ╣äņČöņ¢┤ Ļ░Ćņן ņĀüĒĢ®ĒĢ£ ņśłņĖĪĻ░ÆņØä ņČöļĪĀĒĢśļŖö Ļ▓āņØ┤ļŗż. ļ╣äņ¦ĆļÅäĒĢÖņŖĄņØĆ ļĀłņØ┤ļĖöņØ┤ ņŚåļŖö ļŹ░ņØ┤Ēä░ļź╝ ĒāÉņāēĒĢśļ®░, ĻĄ¼ņĪ░ļéś Ēī©Ēä┤ņØä ņ░ŠĻ▒░ļéś ņ░©ņøÉņØä ņČĢņåīĒĢśļŖö(ņĀĢļ│┤ļ¤ēņØ┤ ņāüļīĆņĀüņ£╝ļĪ£ ņĀüņØĆ ļ│ĆņłśļōżņØä ļ░░ņĀ£ĒĢśĻ│Ā ņĀäņ▓┤ ļŹ░ņØ┤Ēä░ļź╝ ņל ņäżļ¬ģĒĢśļŖö ņØ╝ļČĆ ļ│Ćņłśļōżļ¦ī ļé©ĻĖ░Ļ▒░ļéś ņäżļ¬ģļĀźņØ┤ ļåÆņØĆ ļ│Ćņłśļź╝ ņāłļĪ£ ņāØņä▒ĒĢśņŚ¼ ņĀäņ▓┤ ļ│Ćņłś ņłśļź╝ ņżäņØ┤ļŖö) ņ×æņŚģņØä ņłśĒ¢ēĒĢ£ļŗż. ņżĆņ¦ĆļÅäĒĢÖņŖĄņØĆ ņ¦ĆļÅäĒĢÖņŖĄĻ│╝ ļ╣äņ¦ĆļÅäĒĢÖņŖĄļ░®ņŗØņØä ĒĢ©Ļ╗ś ĒÖ£ņÜ®ĒĢśņŚ¼, ļīĆĻĘ£ļ¬© ļŹ░ņØ┤Ēä░ņŚÉņä£ ņØ╝ļČĆ ļŹ░ņØ┤Ēä░ņŚÉļ¦ī ļĀłņØ┤ļĖöņØ┤ ņĀ£ņŗ£ļÉśņ¢┤ ņ׳ņØä Ļ▓ĮņÜ░ ņ£ĀņÜ®ĒĢĀ ņłś ņ׳ļŗż. Ļ░ĢĒÖöĒĢÖņŖĄņØĆ ņŻ╝ņ¢┤ņ¦ä ļ│Ąņ×ĪĒĢ£ ĒÖśĻ▓ĮņŚÉ ļīĆĒĢ┤ ĒŖ╣ņĀĢ Ē¢ēļÅÖņØä ņĘ©Ē¢łņØä ļĢī ņŻ╝ņ¢┤ņ¦ĆļŖö ļ│┤ņāü Ēś╣ņØĆ ņåÉņŗżņŚÉ ļīĆĒĢ£ ĒĢÖņŖĄņØä ĒåĄĒĢ┤, ļłäņĀüļ│┤ņāüņØä ņĄ£ļīĆĒÖöĒĢśļŖö ņĄ£ņĀüņØś Ē¢ēļÅÖņØä ĒāÉņāēĒĢśļ®░, ņØ┤ļ¤¼ĒĢ£ ĒĢÖņŖĄņØĆ ņŗżņĀ£ ņ×æņŚģņØä ņ¦äĒ¢ēĒĢśļ®░ ļ░£ņāØĒĢśļŖö Ē¢ēļÅÖ-ļ░śņØæ ļŹ░ņØ┤Ēä░ļź╝ ĒåĄĒĢ┤ ņŗżņŗ£Ļ░äņ£╝ļĪ£ ņØ┤ļŻ©ņ¢┤ņ¦äļŗż. ĒĢ┤Ļ▓░ĒĢśĻ│Āņ×É ĒĢśļŖö ļ¼ĖņĀ£ņŚÉ ļīĆĒĢ┤ ņ¢┤ļ¢ż ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śņØä ņäĀĒāØĒĢĀ Ļ▓āņØĖĻ░ĆņŚÉ ļīĆĒĢ┤ ņØ╝ļČĆ ņ░ĖĻ│Ā Ļ░ĆļŖźĒĢ£ ņ¦Ćņ╣©ļōżņØ┤ ņ׳ĻĖ┤ ĒĢśņ¦Ćļ¦ī(ņśłņŗ£: ŌĆ£cheat-sheetŌĆØ for initial ML estimators, scikitlearn; https://scikit-learn.org/stable/tutorial/machine_ learning_map/index.html), ļīĆļČĆļČäņØś Ļ▓ĮņÜ░ ņĀüņĀłĒĢ£ ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śņØś ņäĀĒāØņØĆ ļŹ░ņØ┤Ēä░ņØś ņ¢æ, ĻĄ¼ņĪ░, ļ¼ĖņĀ£ Ēś╣ņØĆ Ļ░ĆņäżņØś ĒŖ╣ņä▒, ĻĖ░ņĪ┤ ņ¦ĆņŗØ, ņŚ░ĻĄ¼ņ×ÉņØś Ļ▓ĮĒŚśĻ│╝ ņ¦üĻ┤Ć, ĒĢÖņŖĄļÉ£ ņĢīĻ│Āļ”¼ņ”śņØś ņä▒ļŖź ļō▒ņØä Ļ│ĀļĀżĒĢśņŚ¼ ņ×ÉļŻīļź╝ ĒāÉņāēĒĢśĻ│Ā ļ¬©ļŹĖņØä ĻĄ¼ņČĢĒĢśļŖö ļ░śļ│ĄņĀüņØĖ Ļ│╝ņĀĢņØä ĒåĄĒĢ┤ ņØ┤ļŻ©ņ¢┤ņ¦äļŗż(Fig. 1). ņØ┤ļź╝ ņ£äĒĢ┤ ĒĢ┤Ļ▓░ĒĢśĻ│Āņ×É ĒĢśļŖö ļ¼ĖņĀ£ ļ░Å ļŹ░ņØ┤Ēä░ņØś ĒŖ╣ņä▒ņŚÉ ļö░ļØ╝ ļ©ĖņŗĀļ¤¼ļŗØ ļ¬©ļŹĖņŚÉ ļīĆĒĢ£ ņĄ£ņĀü ĒÅēĻ░Ćņ¦ĆĒæ£Ļ░Ć ņŗĀņżæĒ׳ Ļ▓░ņĀĢļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż(Table 2) [8-10].
ļŗ╣ļć©ļ│æ ļ░Å ļé┤ļČäļ╣äņ¦łĒÖś ļ©ĖņŗĀļ¤¼ļŗØ ņĀüņÜ® ĒśäĒÖ®
ņĄ£ĻĘ╝ 5ļģäĻ░ä 611Ļ░£ ņśüļ¼Ė ļģ╝ļ¼Ė(ņØĖĻ░ä ļīĆņāü, ņøÉņĀĆļ¦ī ĒżĒĢ©)ņØś ņĀ£ļ¬®ņØä ļČäņäØĒĢśņŚ¼ ņĀäņ▓┤ 2,155 ļŗ©ņ¢┤ ņżæ Ļ░Ćņן ļ╣łļ▓łĒĢśĻ▓ī ņé¼ņÜ®ļÉ£ 30Ļ░£ ļŗ©ņ¢┤ļź╝ ņČöņČ£ĒĢśņśĆņØä ļĢī, ņ¦łĒÖś ņżæņŚÉņä£ļŖö diabetesļéś diabeticņØ┤ Ļ░Ćņן ĒØöĒĢśĻ▓ī ļō▒ņןĒĢśņśĆņ£╝ļ®░(52%), retinopathy (14%), thyroid (14%)Ļ░Ć ļÆżļź╝ ņØ┤ņŚłļŗż. ļ©ĖņŗĀļ¤¼ļŗØ ļ¬®ņĀüņ£╝ļĪ£ļŖö detection, classification, identification, diagnosis ļō▒ ņ¦äļŗ© Ļ┤ĆļĀ© ļŗ©ņ¢┤Ļ░Ć 40%ļĪ£ Ļ░Ćņן ļ¦ÄņĢśņ£╝ļ®░, risk prediction Ēś╣ņØĆ predictionņØ┤ 31%ļĪ£ ņ░©ņł£ņ£ä, ĻĘĖ ņÖĖ segmentation (5%), Ēś╣ņØĆ bioinformatics (7%) ļō▒ņØ┤ ņ׳ņŚłļŗż. ņØ┤ ņżæ 1) ņ¦ĆļÅä, ļ╣äņ¦ĆļÅä, ņżĆņ¦ĆļÅä, Ēś╣ņØĆ Ļ░ĢĒÖöĒĢÖņŖĄ ĒÖ£ņÜ® ņŗżļĪĆļź╝ ņĀ£Ļ│ĄĒĢĀ ņłś ņ׳ņ£╝ļ®░, 2) ņĄ£ĻĘ╝ 3ļģä ņØ┤ļé┤ ļ░£Ēæ£ļÉ£ ļŗ╣ļć©ļ│æ ņŚ░Ļ┤ĆļČäņĢ╝ ņŚ░ĻĄ¼ 6ĒÄĖņØä Ļ▓ĆĒåĀĒĢśņśĆļŗż. ĒĢ┤ļŗ╣ ņŚ░ĻĄ¼ ņäĖļČĆ ļé┤ņÜ®ņØĆ Table 3ņŚÉ ņĀ£ņŗ£ĒĢśņśĆļŗż[4,5,11-14].
ņäĀļ│äĻ▓Ćņé¼ ļ░Å ņ¦łĒÖś ņ¦äļŗ©
1. ņäĀļ│äĻ▓Ćņé¼ ņä▒ļŖź Ļ░£ņäĀ
ļ¦ÄņØĆ ņŚ░ĻĄ¼ņ×ÉļōżņØ┤ ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śņØś ĒÖ£ņÜ®ņØ┤ ļŗ╣ļć©ļ│æ ļ░Å ļé┤ļČäļ╣äņ¦łĒÖśņØś ņäĀļ│äĻ▓Ćņé¼ ņä▒ļŖźĻ░£ņäĀņŚÉ ļÅäņøĆņØä ņżä ņłś ņ׳ņØäņ¦Ć ņŚ░ĻĄ¼ĒĢ┤ņÖöļŗż. Artzi ļō▒[4]ņØĆ ņĀäņ×ÉņØśļ¼┤ĻĖ░ļĪØ EHR ļŹ░ņØ┤Ēä░ļ▓ĀņØ┤ņŖżļź╝ ĒåĀļīĆļĪ£ ņ×äņŗĀņä▒ļŗ╣ļć©ļ│æņØä ņäĀļ│äĻ▓Ćņé¼ĒĢśļŖö ņĢīĻ│Āļ”¼ņ”śņØä Ļ░£ļ░£ĒĢśņśĆļŗż. 2010ļģäļČĆĒä░ 2017ļģäļÅäĻ╣īņ¦Ć ņØ┤ņŖżļØ╝ņŚś 36ļ¦īņŚ¼ ļ¬ģņØś ņ×äņé░ļČĆļĪ£ļČĆĒä░ ņłśņ¦æļÉ£ 58ļ¦īĻ▒┤ņØś EHR ņ×ÉļŻīļź╝ ĒÖ£ņÜ®ĒĢśņŚ¼ ņ×äņŗĀņä▒ļŗ╣ļć©ļ│æ ņäĀļ│äĻ▓Ćņé¼ ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śņØä ĒĢÖņŖĄņŗ£ņ╝░ļŗż. 2,355Ļ░£ņØś Ēøäļ│┤ ļ│Ćņłś ņżæ, ņŚ░ĻĄ¼ņ×ÉļōżņØĆ gradient boosting model ĻĖ░ļ░śņ£╝ļĪ£ 9Ļ░£ņØś ņ×ÉĻ░ĆņØæļŗĄņØ┤ Ļ░ĆļŖźĒĢ£ ļ│Ćņłśļ¦īņØä ĒÖ£ņÜ®ĒĢ£ ļ¬©ļŹĖņØä ļ¦īļōżņŚłĻ│Ā ņØ┤ļŖö ĻĖ░ņĪ┤ ņäĀļ│äĻ▓Ćņé¼ ļ░®ļ▓ĢņØĖ 24~28ņŻ╝ ņé¼ņØ┤ ļŗ╣ļČĆĒĢśĻ▓Ćņé¼ņŚÉ ļ╣äĒĢ┤ ļŹö ņĪ░ĻĖ░ņŚÉ ņŗ£Ē¢ēĒĢĀ ņłś ņ׳ņ£╝ļ®┤ņä£ļÅä ņóŗņØĆ ņä▒ļŖźņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż(area under the receiver operating characteristics curve, 0.80 vs. 0.68).
2. ņ¦äļŗ©ļ▓Ģ Ļ░£ņäĀ
ņל ĻĄ¼ņČĢļÉśĻ│Ā Ļ▓Ćņ”ØļÉ£, ņĀĢĒÖĢĒĢ£ ļ©ĖņŗĀļ¤¼ļŗØ ļ¬©ļŹĖņØĆ ĻĖ░ņĪ┤ņØś ņ╣©ņŖĄņĀü Ļ▓Ćņé¼ļź╝ ļīĆņ▓┤ĒĢĀ ņłś ņ׳ļŖö Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŗż. ņØ╝ļĪĆļĪ£ ļ╣äņĢīņĮ£ņä▒ņ¦Ćļ░®Ļ░ä(non-alcoholic fatty liver disease, NAFLD)ņØĆ ņĀäņäĖĻ│äņĀüņ£╝ļĪ£ ĻĖēņåŹĒ׳ ņ£Āļ│æļźĀņØ┤ ņ”ØĻ░ĆĒĢśĻ│Ā ņ׳ļŖö ņ¦łĒÖśņØ┤ņ¦Ćļ¦ī, ņŚ¼ņĀäĒ׳ ņĪ░ņ¦üņāØĻ▓ĆņØ┤ ĒÖĢņ¦äņØś gold standardļĪ£ ļÉśņ¢┤ ņ׳ņ¢┤ ņ¦äļŗ©Ļ│╝ņĀĢņØś ļČĆļŗ┤ņØä ņ┤łļלĒĢ£ļŗż. ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ Ēśłņ▓Łņ£╝ļĪ£ļČĆĒä░ ļČäņäØĒĢ£ lipidomic, glycomic, liver fatty acid ļŹ░ņØ┤Ēä░ļź╝ ĒÖ£ņÜ®, support vector machine ĻĖ░ļ░ś NAFLD ņ¦äļŗ© ņĢīĻ│Āļ”¼ņ”śņØä ņĀ£ņŗ£ĒĢśņśĆļŗż[11]. Ļ░äņä¼ņ£ĀĒÖö ņĪ┤ņ×¼ ņŚ¼ļČĆņŚÉ ļīĆĒĢśņŚ¼, ĒĢ┤ļŗ╣ ļ¬©ļŹĖņØĆ 10Ļ░£ņØś ļŗ©ņł£ĒĢ£ lipid speciesļź╝ ĒÖ£ņÜ®ĒĢ£ ļ¬©ļŹĖļĪ£ļÅä 98%ņŚÉ ļŗ¼ĒĢśļŖö ņĀĢĒÖĢļÅäļź╝ ļ│┤ņŚ¼ņŻ╝ņ¢┤, lipidomicsņŚÉ ĻĖ░ļ░śĒĢ£ ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śņØ┤ Ļ░äņāØĻ▓ĆņŚÉ ļīĆĒĢ£ ļīĆņĢłņØ╝ ņłś ņ׳ļŖö Ļ░ĆļŖźņä▒ņØä ņĀ£ņŗ£ĒĢśņśĆļŗż. ļŗżļ¦ī, ņØ┤ļ¤¼ĒĢ£ ņĢīĻ│Āļ”¼ņ”śņØĆ Ļ░£ļ░£ņŚÉ ĒÖ£ņÜ®ļÉ£ ļŹ░ņØ┤Ēä░ņģŗņØś ĻĘ╝ļ│ĖņĀüņØĖ ņĪ░Ļ▒┤(ņØĖņóģ ļō▒)ņŚÉ ĻĄŁĒĢ£ļÉśņ¢┤ ļŗżļźĖ ņØĖĻĄ¼ņ¦æļŗ©ņŚÉņä£ņØś ņČöĻ░Ć Ļ▓Ćņ”ØņØ┤ ļ░śļō£ņŗ£ ĒĢäņÜöĒĢśļ®░ ĒĢ┤ļŗ╣ ņĢīĻ│Āļ”¼ņ”śņØś Ļ▓ĮņÜ░ Ļ▓Įņ”ØņØś NAFLDņŚÉ ļīĆĒĢ┤ņä£ļÅä ņóŗņØĆ ņä▒ļŖźņØä ĒÖĢļ│┤ĒĢĀ ņłś ņ׳ņØäņ¦ĆņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼Ļ░Ć ņČöĻ░ĆļĪ£ ĒĢäņÜöĒĢśļŗż[15].
ņ£äĒŚśļÅä ņśłņĖĪ
1. ņ×äņāüĻ▓ĮĻ│╝ ņśłņĖĪ
ņĀĢĒÖĢĒĢ£ ņ×äņāüĻ▓ĮĻ│╝ ņśłņĖĪņØĆ Ļ░£ļ│äĒÖöļÉ£ ņ╣śļŻī ļ░Å Ļ┤Ćļ”¼ļź╝ Ļ░ĆļŖźĒĢśĻ▓ī ĒĢ£ļŗżļŖö ņĀÉņŚÉņä£ ņżæņÜöĒĢśļŗż. WATCH-DM scoreļŖö ņĀ£2ĒśĢ ļŗ╣ļć©ļ│æ ĒÖśņ×ÉņŚÉņä£ ņŗ¼ļČĆņĀä ļ░£ņāØ ņ£äĒŚśļÅäļź╝ ņśłņĖĪĒĢśļŖö ļ©ĖņŗĀļ¤¼ļŗØ ļ¬©ļŹĖļĪ£, ĻĖ░ņĪ┤ ņל ņĢīļĀżņ¦ä ļ¼┤ņ×æņ£äļīĆņĪ░ĻĄ░ ņŚ░ĻĄ¼ņØĖ ACCORD ņŚ░ĻĄ¼ņ×ÉļŻīņŚÉņä£ ļ¬©ļŹĖņØä ĒĢÖņŖĄņŗ£ĒéżĻ│Ā ļśÉ ļŗżļźĖ ļīĆĻĘ£ļ¬© ļ¼┤ņ×æņ£äļīĆņĪ░ĻĄ░ ņŚ░ĻĄ¼ņ×ÉļŻīņØĖ ALLHAT ņŚ░ĻĄ¼ņ×ÉļŻīņŚÉņä£ ņÖĖļČĆĻ▓Ćņ”Ø(external validation)ņØä ņŗ£Ē¢ēĒĢśņŚ¼, ņŗĀļó░ĒĢĀļ¦īĒĢ£ ļ¬©ļŹĖņØś ņä▒ļŖźņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[12]. Random survival forest ĻĖ░ļ░ś ļ©ĖņŗĀļ¤¼ļŗØ ļ¬©ļŹĖĻ│╝ ĒĢ©Ļ╗ś, ņ×äņāüņØśņé¼ņŚÉĻ▓ī ņ╣£ņłÖĒĢ£ ņĀÉņłś ĻĖ░ļ░ś Ļ│äņé░Ēæ£ļź╝ ņĀ£ņŗ£ĒĢśņŚ¼ ņŚ¼ļ¤¼ ĒÖśĻ▓ĮņŚÉņä£ ĒÖ£ņÜ®ĒĢĀ ņłś ņ׳ļŖö ņ£äĒŚśļÅä ņśłņĖĪ ļ¬©ļŹĖņØä ņĀ£ņŗ£ĒĢśņŚ¼ ļ©ĖņŗĀļ¤¼ļŗØņØä ĒÖ£ņÜ®ĒĢ£ ņóŗņØĆ ņ×äņāüņŚ░ĻĄ¼ņØś Ēæ£ļ│ĖņØä ļ│┤ņŚ¼ņŻ╝Ļ│Ā ņ׳ļŗż.
2. ņ╣śļŻīļ░śņØæ ņśłņĖĪ
ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śņØä ĒåĄĒĢ┤ ĻĖ░ņĪ┤ ņŚ░ĻĄ¼ļ░®ņŗØņ£╝ļĪ£ ĒāÉņāēĒĢśĻĖ░ ņ¢┤ļĀżņøĀļŹś ļŗżņ¢æĒĢ£ ņ╣śļŻīļ░śņØæĻĄ░ņØä Ļ░£ļ│äĒÖöĒĢśņŚ¼ ņśłņĖĪĒĢĀ ņłś ņ׳ļŖö Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŗż. ņŚ░ĻĄ¼ņ×ÉļōżņØĆ ACCORD ņŚ░ĻĄ¼ņ×ÉļŻīļź╝ Ļ▓ĆĒåĀĒĢśņŚ¼, ĻĖ░ņĪ┤ Ēæ£ņżĆ Ēśłļŗ╣Ļ┤Ćļ”¼ ļīĆļ╣ä ņ¦æņżæņĀüņØĖ Ēśłļŗ╣Ļ┤Ćļ”¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆņØä ļĢī ļ│┤ņØ┤ļŖö ļŗżņ¢æĒĢ£ ļ░śņØæĻĄ░ņØä ņ×¼ļČäņäØĒĢśņśĆļŗż. ļ╣äļĪØ 2008ļģäļÅä ļ░£Ēæ£ļÉ£ ACCORD ņŚ░ĻĄ¼ņØś Ļ▓░ļĪĀņØĆ ņ¦æņżæĒśłļŗ╣Ļ┤Ćļ”¼Ļ░Ć Ēæ£ņżĆņ╣śļŻīļ▓ĢņŚÉ ļ╣äĒĢ┤ ņé¼ļ¦ØļźĀņØä ņ”ØĻ░Ćņŗ£Ēé©ļŗżļŖö Ļ▓āņØ┤ņŚłņ¦Ćļ¦ī, ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śņØä ĒåĄĒĢ£ ņé¼ĒøäļČäņäØņŚÉņä£ ņŚ░ĻĄ¼ņ×ÉļōżņØĆ ņ¦æņżæĒśłļŗ╣Ļ┤Ćļ”¼Ļ░Ć ņŗżņĀ£ ņé¼ļ¦ØļźĀ Ļ░£ņäĀņŚÉ ņ£ĀņØĄĒ¢łļŹś ļīĆņāüĻĄ░ņØä ņ░ŠņØä ņłś ņ׳ņŚłņ£╝ļ®░, ņāüļīĆņĀüņ£╝ļĪ£ ņé¼ļ¦ØļźĀ ņ”ØĻ░ĆņŚÉ ņśüĒ¢źņØä ņżĆ Ļ│Āņ£äĒŚśĻĄ░ņØĆ ņĀäņ▓┤ ļīĆņāüĻĄ░ ņżæņŚÉņä£ ņåīņłśņ×äņØä ņĀ£ņŗ£ĒĢśņŚ¼ ĻĖ░ņĪ┤ ņŚ░ĻĄ¼Ļ▓░Ļ│╝ļź╝ ņ×¼ĒĢ┤ņäØĒĢĀ ņłś ņ׳ļŖö Ļ░ĆļŖźņä▒ņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż[13]. ņØ┤ ņŚ░ĻĄ¼ļŖö ĻĖ░ņĪ┤ ļīĆĻĘ£ļ¬© ļ¼┤ņ×æņ£äļīĆņĪ░ĻĄ░ ņŚ░ĻĄ¼ņØś Ļ▓░Ļ│╝Ļ░Ć ņŗĀņżæĒĢśĻ▓ī ĒĢ┤ņäØļÉĀ ĒĢäņÜöĻ░Ć ņ׳ņ£╝ļ®░, ļ©ĖņŗĀļ¤¼ļŗØņØä ĒÖ£ņÜ®ĒĢśņŚ¼ ļÅÖņØ╝ņ╣śļŻīļ▓ĢņŚÉ ļīĆĒĢ┤ ļŗżņ¢æĒĢ£ ņ╣śļŻīļ░śņØæņØä ļ│┤ņØ╝ ņłś ņ׳ļŖö ļ╣äĻĘĀņ¦łĒĢ£ ņ¦æļŗ©ņØä ņ░ŠņĢäļé┤Ļ│Ā ņØ┤ņŚÉ ļ¦×ņČś Ļ░£ļ│äĒÖöļÉ£ ņ╣śļŻīņĀü ņĀæĻĘ╝ņØä Ļ│ĀļĀżĒĢĀ ņłś ņ׳ņØīņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż. ĒĢ£ ņŚ░ĻĄ¼ļŖö Ļ░ĢĒÖöĒĢÖņŖĄņØä ĒåĄĒĢ┤ ņĀ£1ĒśĢ ļŗ╣ļć©ļ│æ ĒÖśņ×ÉņŚÉņä£ ņÜ┤ļÅÖļ¤ē, ņŗØņØ┤ļ¤ē ļō▒ ļ│ĆĒÖöĒĢśļŖö ĒÖśĻ▓ĮņĪ░Ļ▒┤ņØä ļ░śņśüĒĢśņŚ¼ ņØĖņŖÉļ”░ ĒĢäņÜöļ¤ē Ļ▓░ņĀĢņØä ļÅäņÜĖ ņłś ņ׳ļŖö Ļ░ĆļŖźņä▒ņØä ņĀ£ņŗ£ĒĢśņśĆļŗż[5]. ņĢäņ¦ü ņä▒ļŖźņØ┤ ņČ®ļČäĒĢśņ¦ä ņĢŖņ¦Ćļ¦ī, ņØ┤ļ¤¼ĒĢ£ ņŚ░ĻĄ¼Ļ▓░Ļ│╝ļōżņØĆ ļ©ĖņŗĀļ¤¼ļŗØņØ┤ ņ╣śļŻīļ░śņØæ ņśłņĖĪ ļ░Å ņØ┤ļź╝ ĒåĄĒĢ£ Ļ░£ļ│äĒÖöļÉ£ ņĀæĻĘ╝ņØä Ļ░ĆļŖźĒĢśĻ▓ī ĒĢśļŖö ņżæņÜöĒĢ£ ļÅäĻĄ¼ļĪ£ ĒÖ£ņÜ®ļÉĀ Ļ░ĆļŖźņä▒ņØä ņŗ£ņé¼ĒĢ£ļŗż.
ņżæĻ░£ņŚ░ĻĄ¼
ļ©ĖņŗĀļ¤¼ļŗØ ņĢīĻ│Āļ”¼ņ”śņØĆ Ēśäņ×¼ ņŻ╝ļ¬®ņØä ļ░øĻ│Ā ņ׳ļŖö ļŗżņżæņśżļ»╣ņŖżļź╝ ĻĖ░ļ░śņ£╝ļĪ£ ĒĢ£ ņ×äņāü-ņżæĻ░£ņŚ░ĻĄ¼ņ×ÉļŻī ļČäņäØņŚÉņä£, ņłśļ¦ÄņØĆ ļ│Ćņłśļōż ņżæ ņŻ╝ņÜö ļ│Ćņłśļź╝ ņäĀĒāØĒĢśĻ│Ā ļ¬©ļŹĖņØä ĒÜ©Ļ│╝ņĀüņ£╝ļĪ£ ĻĄ¼ņČĢĒĢśĻĖ░ ņ£äĒĢ£ ņŻ╝ņÜöĒĢ£ ļÅäĻĄ¼ļĪ£ ĒÖ£ņÜ®ļÉĀ ņłś ņ׳ļŗż. Liu ļō▒[14]ņØĆ ņé¼ļ×īņŚÉ ņä£ ņÜ┤ļÅÖ Ēøä Ēśłļŗ╣ ļ│ĆĒÖö ļ░śņØæņä▒Ļ│╝ ņŚ░Ļ┤ĆļÉ£ ņŻ╝ņÜö ņןļé┤ļ»ĖņāØļ¼╝ĻĘĀņ┤Ø ļ░Å ļīĆņé¼ņ▓┤ļź╝ ĒāÉņāēĒĢśĻĖ░ ņ£äĒĢ┤ ļ©ĖņŗĀļ¤¼ļŗØ ņĀæĻĘ╝ļ▓ĢņØä ĒÖ£ņÜ®ĒĢśņśĆļŗż. ņÜ┤ļÅÖļ░śņØæĻĄ░Ļ│╝ ļ╣äļ░śņØæĻĄ░ņØĆ ņןļé┤ņäĖĻĘĀņ┤Ø ļ░Å ļīĆņé¼ņ▓┤ Ēī©Ēä┤ņŚÉ ņ׳ņ¢┤ ņ£ĀņØśĒĢ£ ņ░©ņØ┤ļź╝ ļ│┤ņśĆņ£╝ļ®░, ļČäļ│ĆņØ┤ņŗØņłĀņØä ĒåĄĒĢ┤ ņźÉņŚÉĻ▓ī ņÜ┤ļÅÖļ░śņØæĻĄ░ņØś ņןļé┤ņäĖĻĘĀņ┤Ø Ēī©Ēä┤ņØä ļ¦īļōżņ¢┤ ņŻ╝ņŚłņØä ļĢī ņÜ┤ļÅÖ ļ░Å ņØĖņŖÉļ”░ļ»╝Ļ░ÉļÅä Ļ░£ņäĀņŚÉ ĒÜ©Ļ│╝ļź╝ ļ│┤ņśĆļŗż. Random forest ņĢīĻ│Āļ”¼ņ”śņØĆ ņłśņ▓£ Ļ░£ņØś ņ×Āņ×¼ņĀü Ēøäļ│┤ ĒŖ╣ņä▒ļ│Ćņłśļōż Ļ░ĆņÜ┤ļŹ░ ļ░śņØæĻĄ░Ļ│╝ ļ╣äļ░śņØæĻĄ░ņØä Ļ░Ćņן ņל Ļ░Éļ│äĒĢśļŖö 29Ļ░£ņØś ĒŖ╣ņä▒ļ│Ćņłś(ņןļé┤ļ»ĖņāØļ¼╝ 14ņóģ, 15Ļ░£ ļīĆņé¼ņ▓┤) ņĪ░ĒĢ®ņØä ņ░ŠņĢśņ£╝ļ®░, ņØ┤ļ¤¼ĒĢ£ ĒŖ╣ņä▒ļ│ĆņłśņØś ņĪ░ĒĢ®ņØĆ ņÜ┤ļÅÖļ░śņØæĻĄ░Ļ│╝ ļ╣äļ░śņØæĻĄ░ņØä ņśłņĖĪĒĢśĻ│Ā ņØ┤ņŚÉ ļö░ļźĖ ņ╣śļŻīņĀäļץņØä ņäĖņÜĖ ņłś ņ׳ļŖö Ļ░£ļ│äĒÖöļÉ£ ņĀæĻĘ╝ņØä ņ£äĒĢ£ ļ░öņØ┤ņśżļ¦łņ╗żļĪ£ ĻĖ░ļŖźĒĢĀ Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŗż.
ĻĄŁļé┤ ļ©ĖņŗĀļ¤¼ļŗØ ĒÖ£ņÜ® ļŗ╣ļć©ļ│æ ņŚ░ĻĄ¼
ĻĄŁļé┤ ļ©ĖņŗĀļ¤¼ļŗØ ĒÖ£ņÜ® ņØśĒĢÖņŚ░ĻĄ¼ļŖö ļöźļ¤¼ļŗØ ĻĖ░ļ▓ĢņØś ļ░£ņĀäĻ│╝ ĒĢ©Ļ╗ś ņŻ╝ļĪ£ ņśüņāüņØśĒĢÖ ļČäņĢ╝ņŚÉņä£ ĒÖ£ļ░£ĒĢśĻ▓ī ņØ┤ļŻ©ņ¢┤ņĪīĻ│Ā, ļŗ╣ļć©ļ│æ ļ░Å ļé┤ļČäļ╣äņ¦łĒÖś ņ×äņāüņŚ░ĻĄ¼ņŚÉņä£ļÅä ņĄ£ĻĘ╝ ņĀüĻĘ╣ņĀüņ£╝ļĪ£ ļ©ĖņŗĀļ¤¼ļŗØņØä ĒÖ£ņÜ®ĒĢśļĀżļŖö ņŚ░ĻĄ¼ņ×ÉļōżņØ┤ ļŖśņ¢┤ļéśĻ│Ā ņ׳ļŗż. ļ│æņøÉņ×ÉļŻī ĻĖ░ļ░śņ£╝ļĪ£ 5ļģä ļé┤ ļŗ╣ļć©ļ░£ņāØļźĀņØä ņśłņĖĪĒĢśļŖö ļ¬©ļŹĖņØä ņĀ£ņŗ£ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö, ņĀäņ×ÉņØśļ¼┤ĻĖ░ļĪØ ĻĖ░ļ░ś 28Ļ░£ ļ│Ćņłśļź╝ ņČöņČ£ĒĢśņŚ¼ ļ©ĖņŗĀļ¤¼ļŗØ ļ¬©ļŹĖņØä ļ¦īļōżĻ│Ā ļŗ╣ļć©ļ│æ ļ░£ņāØ ņŚ¼ļČĆļź╝ ņśłņĖĪĒĢśņśĆļŗż. ļŗżļ¦ī ņśłņĖĪļĀźņŚÉ ņ׳ņ¢┤ņä£ ĻĖ░ņĪ┤ ņśłņĖĪļ¬©ļŹĖņØä ņāüĒÜīĒĢśļŖö ņä▒ļŖźņØä ļ│┤ņŚ¼ņŻ╝ņ¦ĆļŖö ļ¬╗ĒĢśņŚ¼, ĻĖ░ņĪ┤ ļ│æņøÉņ×ÉļŻīņŚÉņä£ ņ¢╗ņØä ņłś ņ׳ļŖö ņśłņĖĪļĀźņØś ĒĢ£Ļ│äļź╝ ļäśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņČöĒøä ĒÖśņ×ÉņØś ņāØĒÖ£Ēī©Ēä┤ņØ┤ļéś ņŗØņŖĄĻ┤Ć, ņÜ┤ļÅÖ ļō▒ ļ│æņøÉ ļ░¢ņŚÉņä£ ņłśņ¦æļÉĀ ņłś ņ׳ļŖö ĒŖ╣ņä▒ļ│ĆņłśņØś ĒÖ£ņÜ®ņØ┤ ņżæņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż[16]. ņĄ£ĻĘ╝ ĒÖ£ņÜ®ņØ┤ ņ”ØĻ░ĆĒĢśĻ│Ā ņ׳ļŖö ņŚ░ņåŹĒśłļŗ╣ņĖĪņĀĢĻĖ░(continuous glucose monitoring, CGM)ņŚÉņä£ ņ¢╗ņØä ņłś ņ׳ļŖö Ēśłļŗ╣ ļ│ĆĒÖö ņŗ£Ļ│äņŚ┤ ļŹ░ņØ┤Ēä░ļŖö ļ©ĖņŗĀļ¤¼ļŗØņØä ĒÖ£ņÜ®ĒĢśĻĖ░ņŚÉ ņĀüņĀłĒĢ£ ņ×ÉļŻīņØ┤ļŗż. ĒĢ£ ĻĄŁļé┤ ņŚ░ĻĄ¼ņŚÉņä£, ņŚ░ĻĄ¼ņ¦äņØĆ 30ļČä ņØ┤ļé┤ ņĀĆĒśłļŗ╣ņØ┤ ļ░£ņāØĒĢĀ Ļ▓āņØä ņśłņĖĪĒĢśļŖö ļ¬©ļŹĖņØä ĻĄ¼ņČĢĒĢśņśĆļŗż. Random forest ļ¬©ļŹĖņØĆ area under the receiver-operating characteristics curve 0.966, ļ»╝Ļ░ÉļÅä 89.6%, ĒŖ╣ņØ┤ļÅä 91.3%ļĪ£ ņóŗņØĆ ņśłņĖĪ ļŖźļĀźņØä ļ│┤ņŚ¼ ņČöĒøä CGM ļ░Å ņØĖĻ│ĄņĘīņן Ļ░£ļ░£, Ļ│ĀļÅäĒÖöņŚÉ ļÅäņøĆņØä ņżä Ļ░ĆļŖźņä▒ņØ┤ ņĀ£ņŗ£ĒĢśņśĆļŗż[17].
Ļ▓░ļĪĀ
ļ©ĖņŗĀļ¤¼ļŗØņØś ĒÖ£ņÜ®ņØĆ ļŹ░ņØ┤Ēä░ ĒÖ£ņÜ®, ĒĢ┤ņäØņŚÉ ņ׳ņ¢┤ ņāłļĪ£ņÜ┤ Ļ░ĆļŖźņä▒ņØä ņĀ£ņŗ£ĒĢśļ®░ ļŗ╣ļć©ļ│æ ļ░Å ļīĆņé¼ņ¦łĒÖś ņŚ░ĻĄ¼ņŚÉ ļÅäņøĆņØä ņżä Ļ░ĆļŖźņä▒ņØ┤ ņ׳ņ¦Ćļ¦ī, Ēśäņ×¼ ņØśļŻīļŹ░ņØ┤Ēä░ņØś ļ│Ąņ×Īņä▒, ļČĆņĀĢĒÖĢņä▒, ņ×Āņ×¼ņĀü ņśżļźśļź╝ Ļ│ĀļĀżĒĢĀ ļĢī ļīĆĻĘ£ļ¬© ņ×ÉļŻīņØś ĒÖĢļ│┤ņÖĆ ļ©ĖņŗĀļ¤¼ļŗØņØś ņĀüņÜ®ņØĆ ņŗĀņżæĒĢ£ ņĀæĻĘ╝ņØ┤ ĒĢäņÜöĒĢśļŗż[18]. ņĀĢĒÖĢĒĢ£ ļ¼ĖņĀ£ ņĀĢņØś Ēś╣ņØĆ Ļ░Ćņäż ņäżņĀĢ, ļŹ░ņØ┤Ēä░ ņ¦ł(quality)ņŚÉ ļīĆĒĢ£ ņ¦ĆņåŹņĀüņØĖ Ļ┤Ćņŗ¼, ņ×äņāüĒśäņן ļ░Å ļ»ĖņČ®ņĪ▒ņłśņÜöņŚÉ ĻĖ░ļ░śĒĢ£ ņŚ░ĻĄ¼ļööņ×ÉņØĖ ļ░Å ļ©ĖņŗĀļ¤¼ļŗØ ņĀäļ¼ĖĻ░Ć ņ╗żļ«żļŗłĒŗ░ņÖĆņØś ņĀüĻĘ╣ņĀüņØ┤Ļ│Ā Ēł¼ļ¬ģĒĢ£ ĒśæļĀźņØ┤ ļ©ĖņŗĀļ¤¼ļŗØņØä ĒåĄĒĢ£ ļŗ╣ļć©ļ│æ ļ░Å ļīĆņé¼ņ¦łĒÖś ņŚ░ĻĄ¼ļź╝ ņä▒Ļ│ĄņĀüņ£╝ļĪ£ ņŗ£Ē¢ēĒĢĀ ņłś ņ׳ļŖö ņżæņÜöĒĢ£ ņÜöņåīĻ░Ć ļÉĀ ņłś ņ׳ļŗż[19]. ļ©ĖņŗĀļ¤¼ļŗØņØä ļŗ╣ļć©ļ│æĻ│╝ ļé┤ļČäļ╣äņ¦łĒÖś ņŚ░ĻĄ¼ņŚÉ ĒÜ©Ļ│╝ņĀüņ£╝ļĪ£ ņĀüņÜ®ĒĢśņŚ¼ ņ×äņāüņĀüņ£╝ļĪ£ ņ£ĀņÜ®ĒĢ£ Ļ▓░Ļ│╝ļź╝ ņØ┤ļüīņ¢┤ļé┤ĻĖ░ ņ£äĒĢ┤ņä£ļŖö, ļīĆĻĘ£ļ¬©, Ļ│ĀĒÆłņ¦łņØś ņØśļŻīļŹ░ņØ┤Ēä░ņØś ĻĄ¼ņČĢ ļ░Å ņĀæĻĘ╝ņä▒ ĒÖĢļ│┤Ļ░Ć ņżæņÜöĒĢśļŗż. ņØ┤ļź╝ ņ£äĒĢśņŚ¼ ļ│æņøÉņ×ÉļŻī, ņ¦ĆņŚŁņé¼ĒÜīņĮöĒśĖĒŖĖ, ĒÖśņ×É ļĀłņ¦ĆņŖżĒŖĖļ”¼, Ļ▒┤Ļ░Ģļ│┤ĒŚś ņ▓ŁĻĄ¼ņ×ÉļŻī, Ļ░£ņØĖ ļØ╝ņØ┤ĒöäļĪ£ĻĘĖ ļō▒ ņŚ¼ļ¤¼ ņ×ÉļŻīļōżņØ┤ ņØĄļ¬ģņä▒ņØä ņ£Āņ¦ĆĒĢ£ ņ▒ä ņŚ░Ļ│äļÉ£ ļŗżļ®┤ļŹ░ņØ┤Ēä░ ĻĄ¼ņČĢ, ņĀĢņĀ£ ļ░Å Ļ│ĄĒåĄņ×ÉļŻīļ¬©ļŹĖ ļō▒ņØä ņØ┤ņÜ®ĒĢ£ ĒÜ©ņ£©ņĀüņØĖ ļŗżĻĖ░Ļ┤Ć ņŚ░ĻĄ¼ ļ¬©ļŹĖ ņłśļ”ĮņØ┤ ĒĢäņÜöĒĢśļŗż. ņĀÉņ░© ņ”ØĻ░ĆĒĢśļŖö ļ©ĖņŗĀļ¤¼ļŗØ ĻĖ░ļ░ś ņŚ░ĻĄ¼Ļ▓░Ļ│╝ļōżņØä ņĀĢĒÖĢĒĢśĻ▓ī ņØ┤ĒĢ┤, ļ╣äĒīÉņĀü ĒÅēĻ░Ć Ēøä ņ×äņāüņŚÉ ļÅäņ×ģĒĢśņŚ¼ ņŗżņĀ£ ĒÖśņ×ÉļōżņŚÉĻ▓ī ļÅäņøĆņØä ņżä ņłś ņ׳ļÅäļĪØ ņ¦äļŻīĒśäņןņØä ļ│ĆĒÖöņŗ£ĒéżĻĖ░ ņ£äĒĢ┤ņä£ļŖö, ņĀäļ¼Ėņ×äņāüĻ▓ĮĒŚśņØä ļ│┤ņ£ĀĒĢśĻ│Ā ņ׳ņ£╝ļ®░ ņ×äņāüĒśäņןņØś ļ»ĖņČ®ņĪ▒ņłśņÜöļź╝ ņל ņØĖņ¦ĆĒĢśĻ│Ā ņ׳ļŖö ļŗ╣ļć©ļ│æ ļ░Å ļīĆņé¼ņ¦łĒÖś ļé┤ļČäļ╣ä ņ×äņāüņØśņé¼ņØś ņŚŁĒĢĀņØ┤ ĒĢäņłśņĀüņØ┤ļŗż.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




