

서론
국민건강영양조사(2012~2018년) 결과에 따르면 우리나라 30세 이상 성인의 7명 중 1명(13.8%)이 당뇨병을 가지고 있는 것으로 보고되었다. 당뇨병유병률은 최근 7년 동안 증가하는 경향을 보였고, 연령이 증가함에 따라 증가하는 추세이다. 2012~2018년 국민건강영양조사 통합 자료에 따른 당뇨병과 동반질환을 살펴보면, 당뇨병 유병자 중 약 절반의 환자가 비만(body mass index [BMI] 25 kg/m2 이상)이었고, BMI가 30 kg/m2 이상인 환자도 11.7%이다. 복부비만을 동반한 당뇨병환자는 54%이며, 복부비만율은 여성이 남성보다 높다. 당뇨병환자 중 63.1% 정도는 고혈압을 동반하였고, 65세 이상에서는 74.3%가 고혈압을 동반하였다. 당뇨병환자 중 72.0%가 고콜레스테롤혈증을 동반하였다. 30세 이상 당뇨병 성인에서 고혈압 및 고지질혈증을 모두 동반한 경우는 43.7%이다[1].
대한당뇨병학회 진료지침 7판에서 당뇨병환자의 치료목표는 혈당조절을 통한 합병증 발생 예방임을 제시하였다[2]. 이를 위해 당뇨병 진단 초기부터 생활습관 개선을 포함하여 적절한 약물치료가 필요하다. 무엇보다도 임상영양요법 교육을 통해 환자 개개인에 적합한 식사관리가 중요하다. 하지만 바쁜 현대 사회에서 시간과 노력이 많이 필요한 당뇨병 식사관리를 꾸준히 실천하고 유지하는 것은 어렵다. 당뇨병 식사요법은 단순히 특정 식품을 제한하거나 식사량을 줄이는 것이 아니다. 적절한 체중을 유지하기 위한 알맞은 양으로, 영양소별로 골고루, 규칙적으로 식사하는 건강한 식습관으로 이해해야 한다.
영양불량이란 영양소섭취의 부족 또는 과잉, 필수 영양소의 불균형 또는 활용 장애를 의미한다. 따라서 본 고에서는 영양불량을 동반한 당뇨병환자에게서 좋은 영양상태를 유지하는 임상영양요법에 대해 알아보고자 한다.
본론
체중 상태는 영양불량을 파악하는 가장 쉬운 방법 중 하나이다. 영양섭취 과잉으로 인한 비만은 뇌혈관질환 위험요인으로 잘 알려져 있지만 이것이 당뇨병이 있는 고령 환자에게 해당되는지 여부는 아직 완전히 밝혀지지 않았다[3]. Tanaka 등[4]은 BMI와 6년간의 관계에 대한 평가에서 J-EDIT (Japanese Elderly Intervention Trial) 참가자의 사망률을 연구하였는데, BMI가 18.5 kg/m2 미만인 사람들은 사망위험이 더 높았고, BMI가 18.5~24.9 kg/m2인 사람들에서 가장 낮은 사망위험이 관찰되었다. 그러나 BMI가 25 kg/m2 이상인 사람들에서는 위험이 증가하지 않았다[4]. Schaap 등[5]의 연구에서는 BMI가 30 kg/m2 이상인 사람들은 계단 오르기를 포함한 보행장애와 기능저하의 위험이 더 높은 것으로 나타났다. 반대로, 낮은 BMI는 노쇠함의 위험요인이다. BMI와 노쇠함의 유병률 사이의 연관성 관계를 확인한 일본 연구에서, BMI가 21.4~25.7 kg/m2인 대상자에서 가장 낮은 노쇠 위험성 관계를 보고하였다[6]. Look AHEAD (Action for Health in Diabetes) 연구의 집중적인 생활 방식 개입 및 체중감소는 당뇨병이 있는 고령자의 장애 발병을 지연시키고 건강 기대수명을 연장했다[7]. 한편, 한국의 40세 이상 환자 코호트에서 BMI가 낮을수록 치매 발병률이 높았다[8].
연구들의 결과를 보았을 때 당뇨병이 있는 고령 환자에서 합병증을 예방하기 위해서는 높은 BMI (≥ 30 kg/m2)를 교정해야 하고 영양실조의 진단기준이기도 한 낮은 BMI (< 18.5 kg/m2)도 피해야 한다[9]. 그러므로 영양불량을 동반한 당뇨병환자의 체중조절을 목표로 열량을 설정할 때에는 환자의 연령, 성별, 체중, 의학적 상태 등을 반드시 고려해야 한다.
MNA (mini nutritional assessment)로 평가된 영양부족 비율은 당뇨병이 없는 노인보다 당뇨병이 있는 노인에서 더 높다[10]. 인지장애, 노쇠 및 사망률의 예방을 위한 노인당뇨병 환자에게 바람직하지 않은 영양상태는 BMI ≥ 30 kg/m2, 체중증가(> 10%), 대사증후군(< 75세), 근감소성 비만, BMI < 18.5 kg/m2, 의도하지 않은 체중감소 및 영양실조이다(Fig. 1) [11].
Fig. 1.
Nutritional states that are not preferred in older patients with diabetes for the prevention of cognitive impairment, frailty, and increased mortality. Adapted from the article of Tamura et al. (Nutrients 2020; 12:3367) [11] under the terms of the Creative Commons Attribution (CC BY 4.0) license. BMI, body mass index; BW, body weight; y.o., years old.

당뇨병환자를 위한 식사요법은 극단적인 식사방법을 권장하지 않는다. 환자 개개인에 맞춘 탄수화물, 단백질, 지방의 식사 계획을 권장한다. 근육 증가와 손실은 단백질 합성과 분해 사이의 균형에 달려 있기 때문에 단백질 회전율의 조절은 근육 항상성에 필수적이다. 과일과 채소, 외인성 항산화 비타민(비타민E, C, 카로티노이드 등)과 미네랄이 풍부한 식단은 골격근 산화환원 항상성을 회복하고 산화 스트레스와 활성산소 및 질소 종의 축적을 방지하여 근육 유지에 기여할 수 있다[12]. 메타분석에 따르면 건강한 식사패턴(과일, 야채 및 통곡물이 많이 함유된 식단)은 65세 이상에서 노쇠 위험을 60% 감소시켰지만 젊은 사람들은 그렇지 않았다[13]. J-ED-IT에 따르면 식사패턴을 건강한 식사패턴(채소와 생선을 많이 섭취), 간식 식사패턴(과자, 과일, 감자를 많이 섭취), 기름진 식사패턴(고기와 지방 과다섭취)으로 구분했다. 75세 이상에서의 사망률은 기름진 식사패턴보다 건강한 식사패턴을 가진 환자에서 낮았다[14]. 한 연구에 따르면 75세 이상의 당뇨병환자는 지중해식 식단에 대한 순응도가 향상되어 걷기와 균형이 개선되었지만 60세에서 74세 사이의 환자에서는 유사한 관계가 관찰되지 않았다[15].
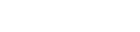
당뇨병환자의 임상영양중재는 대사증후군/비만 치료를 위한 엄격한 식사 제한에서 환자 고령화에 따라 노쇠 및 근감소증 예방을 위한 식사로 전환되어야 한다(Fig. 2) [11]. 특히, 75세 이상의 환자는 단백질, 야채, 과일, 생선이 많이 함유된 식단을 권장한다.
Fig. 2.
Shift in dietary strategies for frailty prevention in older adults with diabetes. Adapted from the article of Tamura et al. (Nutrients 2020; 12:3367) [11] under the terms of the Creative Commons Attribution (CC BY 4.0) license. QOL, quality of life.
대한당뇨병학회 진료지침 7판에서 제시하는 바와 같이 탄수화물, 단백질, 지방섭취의 이상적인 비율은 없다[2]. 임상영양요법은 성별, 연령, 개인의 영양상태에 따라 개별화하여 계획되어야 할 것이다.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




